

Genetic testing offer for inherited neuromuscular diseases within the EURO-NMD reference network: A European survey study
- PMID: 32946487
- PMCID: PMC7500674
- DOI: 10.1371/journal.pone.0239329
Genetic testing offer for inherited neuromuscular diseases within the EURO-NMD reference network: A European survey study
Abstract
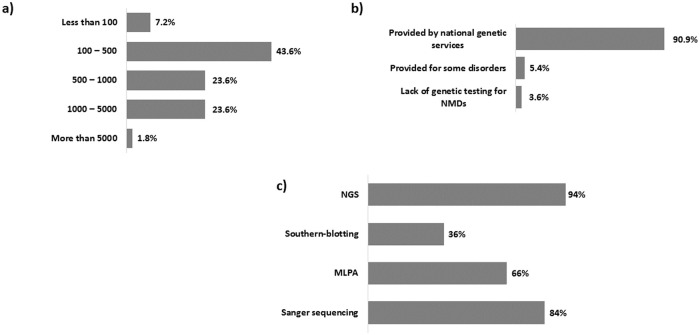
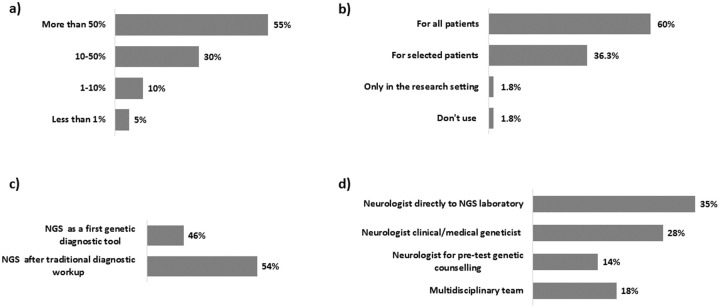
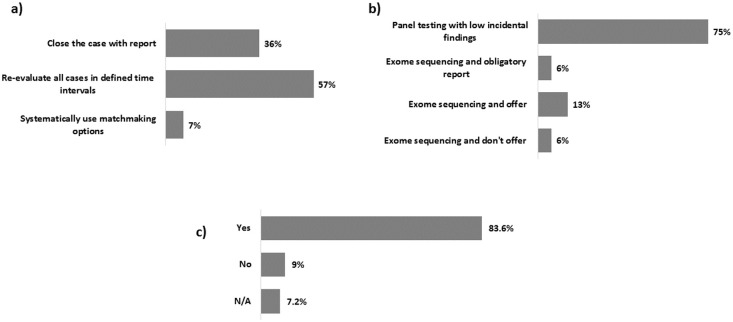
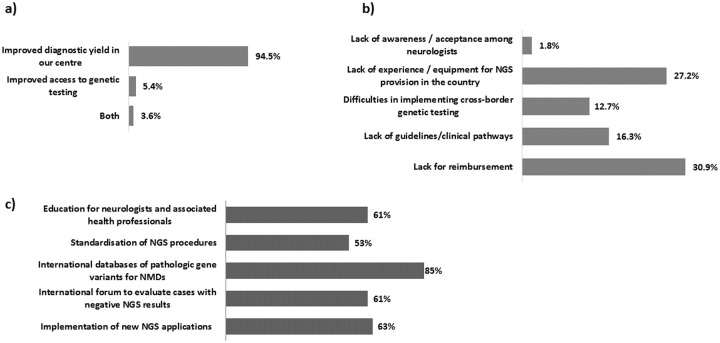
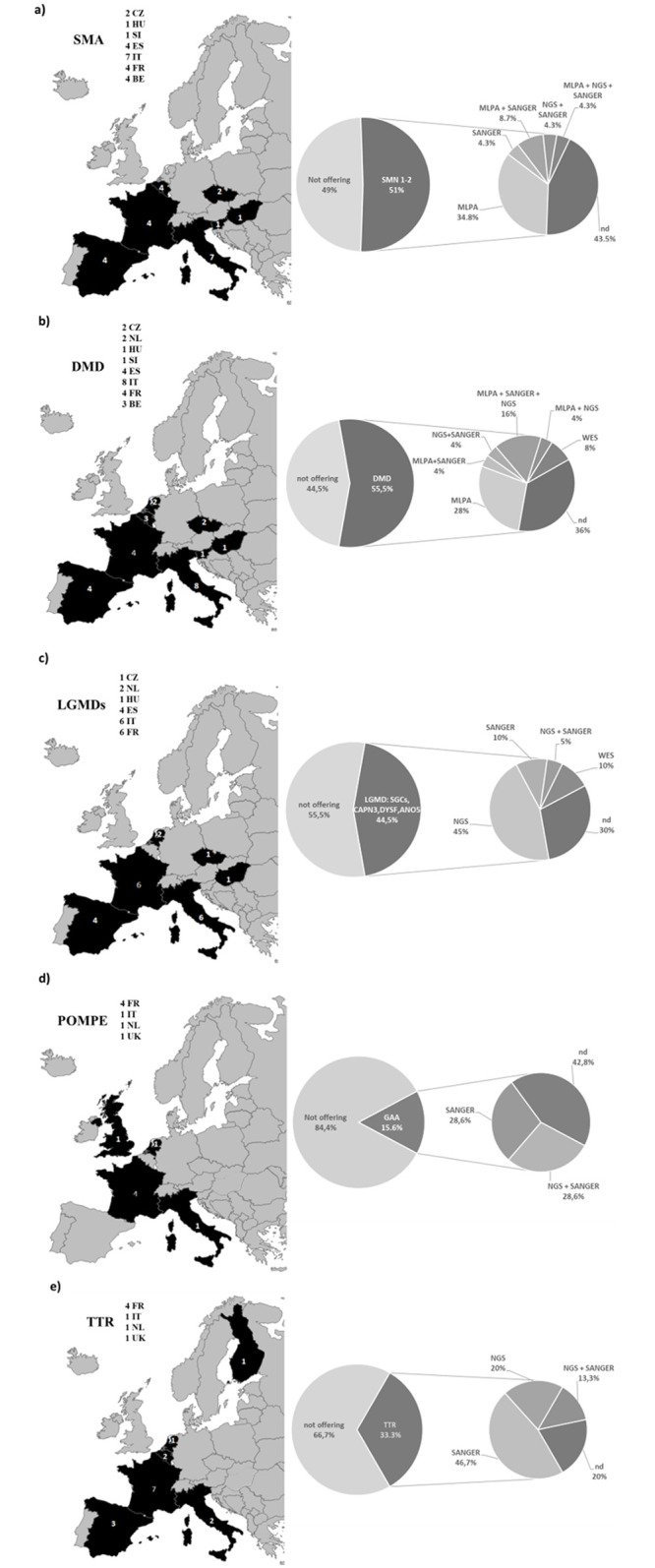
The genetic diagnostics of inherited neuromuscular diseases (NMDs) is challenging due to their clinical and genetic heterogeneity. We launched an online survey within the EURO-NMD European Reference Network (ERN) to collect information about the availability/distribution of genetic testing across 61 ERN health care providers (HCPs). A 17 items questionnaire was designed to address methods used, the number of genetic tests available, the clinical pathway to access genetic testing, the use of next-generation sequencing (NGS) and participation to quality assessment schemes (QAs). A remarkable number of HCPs (49%) offers ≥ 500 genetic tests per year, 43,6% offers 100-500 genetic tests per year, and 7,2% ≤ 100 per year. NGS is used by 94% of centres, Sanger sequencing by 84%, MLPA by 66% and Southern blotting by 36%. The majority of centres (60%) offer NGS for all patients that fulfil criteria for NMD of genetic origin. Pipelines for NGS vary amongst centres, even within the same national system. Referral of patients to genetic laboratories by specialists was frequently reported (58%), and 65% of centres participates in genetic testing QAs. We specifically evaluated how many centres cover SMA, DMD, Pompe, LGMDs, and TTR genes/diseases genetic diagnosis, since these rare diseases benefit from personalised therapies. We used the Orphanet EUGT numbers, provided by 82% of HCPs. SMA, DMD, LGMD, TTR and GAA genes are covered by EUGTs although with different numbers and modalities. The number of genetic tests for NMDs offered across HCPs National Health systems is quite high, including routine techniques and NGS. The number and type of tests offered and the clinical practices differ among centres. We provided evidence that survey tools might be useful to learn about the state-of-the-art of ERN health-related activities and to foster harmonisation and standardisation of the complex care for the rare disease patients in the EU.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Deenen JCW, Horlings CGC, Verschuuren JJGM, Verbeek ALM, Van Engelen BGM. The epidemiology of neuromuscular disorders: A comprehensive overview of the literature. J Neuromuscul Disord. 2015;2(1):73–85. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
