

Diabetes in ageing: pathways for developing the evidence base for clinical guidance
- PMID: 32946822
- PMCID: PMC8223534
- DOI: 10.1016/S2213-8587(20)30230-8
Diabetes in ageing: pathways for developing the evidence base for clinical guidance
Abstract
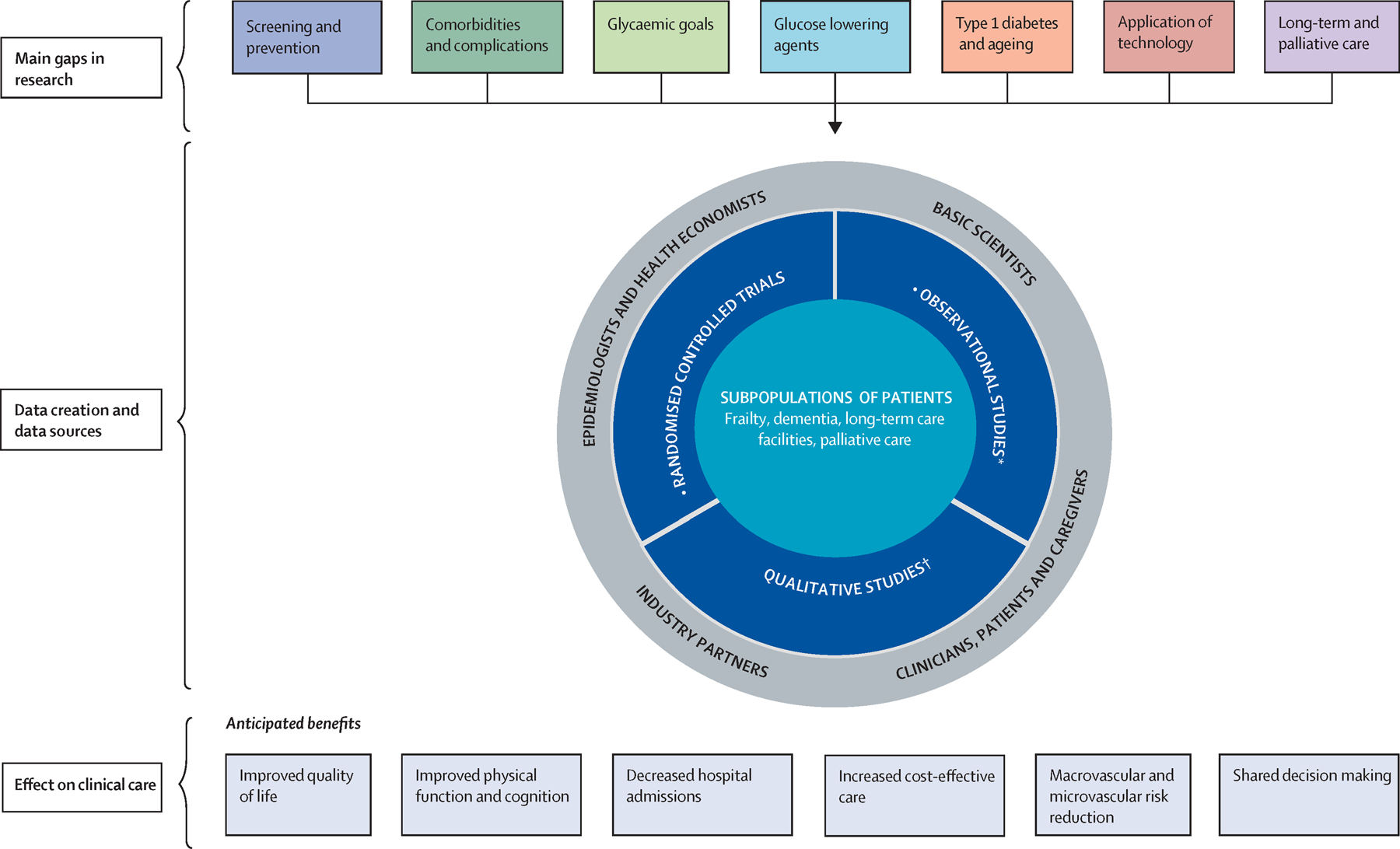
Older adults with diabetes are heterogeneous in their medical, functional, and cognitive status, and require careful individualisation of their treatment regimens. However, in the absence of detailed information from clinical trials involving older people with varying characteristics, there is little evidence-based guidance, which is a notable limitation of current approaches to care. It is important to recognise that older people with diabetes might vary in their profiles according to age category, functional health, presence of frailty, and comorbidity profiles. In addition, all older adults with diabetes require an individualised approach to care, ranging from robust individuals to those residing in care homes with a short life expectancy, those requiring palliative care, or those requiring end-of-life management. In this Review, our multidisciplinary team of experts describes the current evidence in several important areas in geriatric diabetes, and outlines key research gaps and research questions in each of these areas with the aim to develop evidence-based recommendations to improve the outcomes of interest in older adults.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Interest
MNM reports other from Sanofi, other from Lilly, outside the submitted work; GSM reports other from Merck, other from Abbott, other from Novo Nordisk, outside the submitted work. LRM has nothing to disclose. KC reports other from Helmsley Charitable Trust, other from Abbott, other from Adocia, other from Ascensia, other from Apple Pickers Foundation, other from AstraZeneca, other from Becton Dickinson (BD), other from Beta Bionics, other from BigFoot BioMedical, other from Boehringer Ingelheim, other from Boston Consulting Group, other from BrightInsight, a Flex Company, other from Cellnovo, other from CeQur, other from Dexcom, other from Ella Fitzgerald Charitable Foundation, other from Glooko, other from Insulet, other from Intarcia, other from Johnson & Johnson/Janssen, other from Lexicon, other from Lilly, other from Livongo Health, other from MannKind, other from Medtronic, other from Merck, other from Novo Nordisk, other from Onduo, other from Profil (EU & US), other from Prosciento, other from Qualcomm, other from Roche, other from Sanofi, other from Sensionics, other from Tandem, other from WellDoc, other from Xeris, outside the submitted work; PRC reports grants from Department of Veterans Affairs, grants from National Institutes of Health, during the conduct of the study. TCY reports grants from Medtronic, other from MSD, other from Medtronic, other from Sanofi, other from Astra Zeneca, other from Lilly, outside the submitted work. AF has nothing to disclose. OPG reports personal fees from Sanofi, grants and personal fees from Amarin, personal fees from Boehrnger-Ingelheim/Eli Lilly, outside the submitted work. CRK reports personal fees from CohBar, personal fees from Kaleido Bioscience, outside the submitted work. EH reports grants from NIH (NIDDK and NIA), during the conduct of the study. LML reports personal fees from Astra Zeneca, personal fees from Boehringer Ingelheim, personal fees from ConvaTec, personal fees from Dexcom, personal fees from Eli Lilly, personal fees from Insulet, personal fees from Insulogic, personal fees from Janssen Pharmaceuticals, personal fees from Johnson & Johnson, personal fees from Laxmi, personal fees from LifeScan, personal fees from MannKind, personal fees from Medtronic, personal fees from Menarini Diagnostics, personal fees from Merck, personal fees from Novo Nordisk, personal fees from Roche Diagnostics, personal fees from Sanofi, outside the submitted work. CGL has nothing to disclose. SL has nothing to disclose. DMN has nothing to disclose. NP discloses that she is a speaker for Eli Lilly. RP reports speaker and consulting fees from AstraZeneca; consulting fees from Boehringer-Ingelheim; consulting fees from Eisai, Inc.; consulting fees from GlaxoSmithKline; consulting fees from Glytec, LLC; consulting fees from Janssen; grants from Lexicon Pharmaceuticals; grants and consulting fees from Ligand Pharmaceuticals, Inc;, grants and consulting fees from Lilly; grants and consulting fees from Merck; consulting fees from Mundipharma; grants, speaker fees and consulting fees from Novo Nordisk; consulting fees from Pfizer; grants and consulting fees from Sanofi; grants, speaker fees and consulting fees from Takeda; personal consulting fees from Sanofi US Services, Inc., outside the submitted work. Except for consulting fees in February 2018 and June 2018 from Sanofi US Services, Inc., Dr. Richard Pratley’s services were paid for directly to AdventHealth, a nonprofit organization. RG reports and discloses advisory boards of Onduo, Form Health, Vida Health, Lark and Health Reveal. AJS has nothing to disclose.
Figures
References
-
- Sinclair A, Morley JE, Rodriguez-Manas L, Paolisso G, Bayer T, Zeyfang A, et al. Diabetes mellitus in older people: position statement on behalf of the International Association of Gerontology and Geriatrics (IAGG), the European Diabetes Working Party for Older People (EDWPOP), and the International Task Force of Experts in Diabetes. J Am Med Dir Assoc. 2012;13(6):497–502. - PubMed
-
- Benetos A, Novella JL, Guerci B, Blickle JF, Boivin JM, Cuny P, et al. Pragmatic diabetes management in nursing homes: individual care plan. J Am Med Dir Assoc. 2013;14(11):791–800. - PubMed
-
- Mallery LH, Ransom T, Steeves B, Cook B, Dunbar P, Moorhouse P. Evidence-informed guidelines for treating frail older adults with type 2 diabetes: from the Diabetes Care Program of Nova Scotia (DCPNS) and the Palliative and Therapeutic Harmonization (PATH) program. J Am Med Dir Assoc. 2013;14(11):801–8. - PubMed
-
- meneilly GS, Knip A, Tessier D. Canandian Diabetes Association 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada: Diabetes in the elderly. Canadian Journal of Diabetes. 2013;37 (suppl 1):S184–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
