

Pulmonary artery thrombi are co-located with opacifications in SARS-CoV2 induced ARDS
- PMID: 32947171
- PMCID: PMC7483034
- DOI: 10.1016/j.rmed.2020.106135
Pulmonary artery thrombi are co-located with opacifications in SARS-CoV2 induced ARDS
Abstract
Purpose: Patients hospitalized for infection with SARS-CoV-2 typically present with pneumonia. The respiratory failure is frequently complicated by pulmonary embolism in segmental pulmonary arteries. The distribution of pulmonary embolism in regard to lung parenchymal opacifications has not been investigated yet.
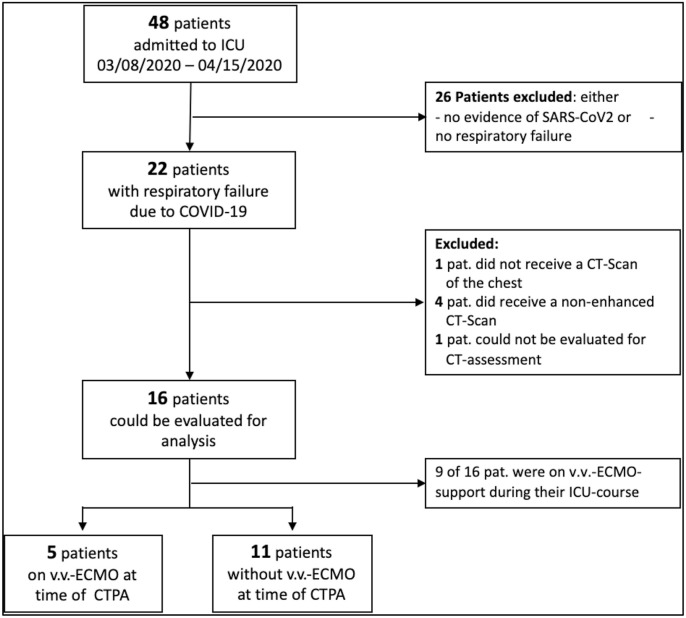
Methods: All patients with COVID-19 treated at a medical intensive care unit between March 8th and April 15th, 2020 undergoing computed tomography pulmonary angiography (CTPA) were included. All CTPA were assessed by two radiologists independently in respect to parenchymal changes and pulmonary embolism on a lung segment basis.
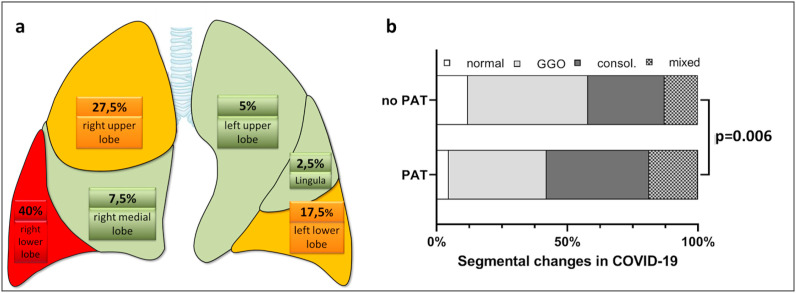
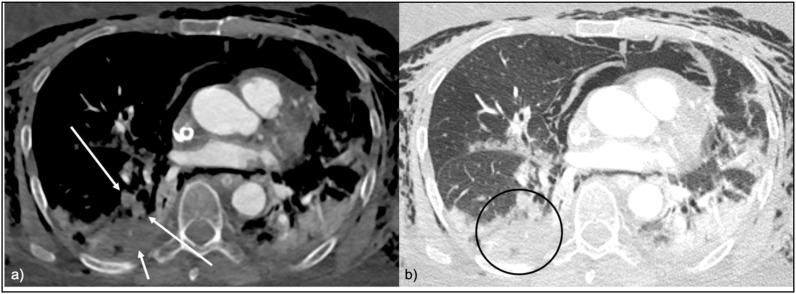
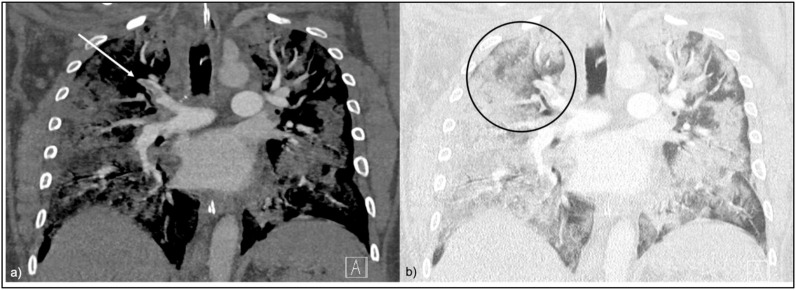
Results: Out of 22 patients with severe COVID-19 treated within the observed time period, 16 (age 60.4 ± 10.2 years, 6 female SAPS2 score 49.2 ± 13.9) underwent CT. A total of 288 lung segment were analyzed. Thrombi were detectable in 9/16 (56.3%) patients, with 4.4 ± 2.9 segments occluded per patient and 40/288 (13.9%) segments affected in the whole cohort. Patients with thrombi had significantly worse segmental opacifications in CT (p < 0.05) and all thrombi were located in opacitated segments. There was no correlation between d-dimer level and number of occluded segmental arteries.
Conclusions: Thrombi in segmental pulmonary arteries are common in COVID-19 and are located in opacitated lung segments. This might suggest local clot formation.
Keywords: COVID19; CT-Scan; CTPA; Pulmonary artery thrombosis; Pulmonary embolism; SARS-CoV2.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflicts of interests.
Figures
Comment in
-
Covid-19 and in situ pulmonary artery thrombosis.Respir Med. 2021 Jan;176:106176. doi: 10.1016/j.rmed.2020.106176. Epub 2020 Oct 2. Respir Med. 2021. PMID: 33092932 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
