

Association between history of cancer and major adverse cardiovascular events in patients with chest pain presenting to the emergency department: a secondary analysis of a prospective cohort study
- PMID: 32947416
- PMCID: PMC7770076
- DOI: 10.1097/MEJ.0000000000000753
Association between history of cancer and major adverse cardiovascular events in patients with chest pain presenting to the emergency department: a secondary analysis of a prospective cohort study
Abstract
Objectives: Cancer survivorship status among patients evaluated for chest pain at the emergency department (ED) warrants high degree of suspicion. However, it remains unclear whether cancer survivorship is associated with different risk of major adverse cardiac events (MACE) compared to those with no history of cancer. Furthermore, while HEART score is widely used in ED evaluation, it is unclear whether it can adequately triage chest pain events in cancer survivors. We sought to compare the rate of MACE in patients with a recent history of cancer in remission evaluated for acute chest pain at the ED to those with no history of cancer, and compare the performance of a common chest pain risk stratification score (HEART) between the two groups.
Methods: We performed a secondary analysis of a prospective observational cohort study of chest pain patients presenting to the EDs of three tertiary care hospitals in the USA. Cancer survivorship status, HEART scores, and the presence of MACE within 30 days of admission were retrospectively adjudicated from the charts. We defined patients with recent history of cancer in remission as those with a past history of cancer of less than 10 years, and currently cured or in remission.
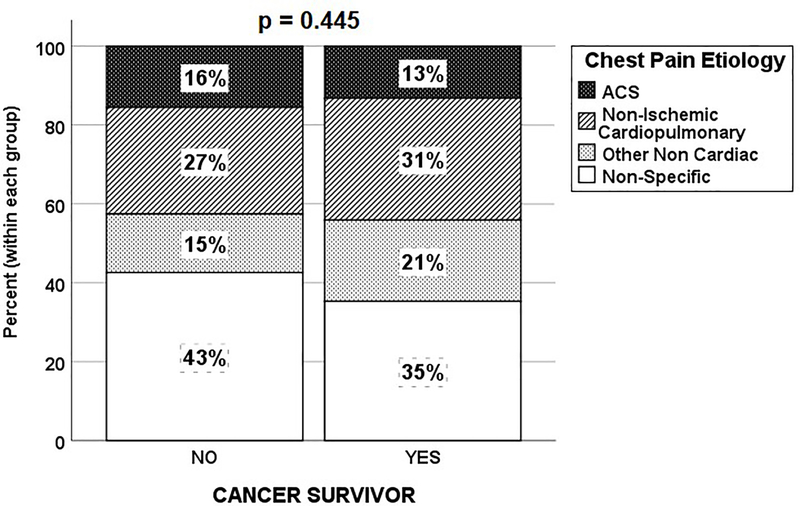
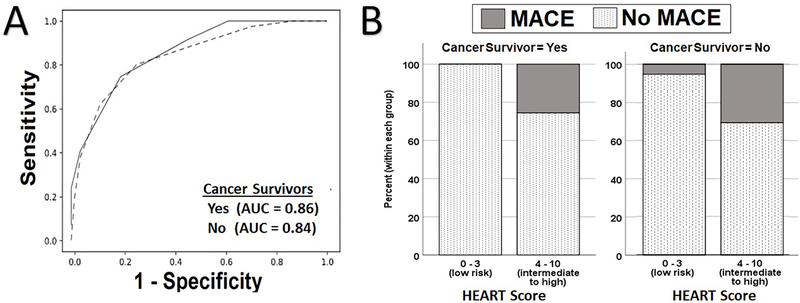
Results: The sample included 750 patients (age: 59 ± 17; 42% females, 40% Black), while 69 patients (9.1%) had recent history of cancer in remission. A cancer in remission status was associated with a higher comorbidity burden, older age, and female sex. There was no difference in risk of MACE between those with a cancer in remission and their counterparts in both univariate [17.4 vs. 19.5%, odds ratio (OR) = 0.87 (95% confidence interval (CI), 0.45-1.66], P = 0.67] and multivariable analysis adjusting for demographics and comorbidities [OR = 0.62 (95% CI, 0.31-1.25), P = 0.18]. Patients with cancer in remission had higher HEART score (4.6 ± 1.8 vs. 3.9 ± 2.0, P = 0.006), and a higher proportion triaged as intermediate risk [68 vs. 56%, OR = 1.67 (95% CI, 1.00-2.84), P = 0.05]; however, no difference in the performance of HEART score existed between the groups (area under the curve = 0.86 vs. 0.84, P = 0.76).
Conclusions: There was no difference in rate of MACE between those with recent history of cancer in remission compared to their counterparts. A higher proportion of patients with cancer in remission was triaged as intermediate risk by the HEART score, but we found no difference in the performance of the HEART score between the groups.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Johnson CB, Davis MK, Law A, Sulpher J. Shared Risk Factors for Cardiovascular Disease and Cancer: Implications for Preventive Health and Clinical Care in Oncology Patients. Can J Cardiol. 2016;32(7):900–907. - PubMed
-
- Geiger S, Lange V, Suhl P, Heinemann V, Stemmler HJ. Anticancer therapy induced cardiotoxicity: review of the literature. Anticancer Drugs. 2010;21(6):578–590. - PubMed
-
- Schimmel KJ, Richel DJ, van den Brink RB, Guchelaar HJ. Cardiotoxicity of cytotoxic drugs. Cancer Treat Rev. 2004;30(2):181–191. - PubMed
-
- Naaktgeboren WR, Linschoten M, de Graeff A, et al. Long-term cardiovascular health in adult cancer survivors. Maturitas. 2017;105:37–45. - PubMed
-
- Cardinale D, Sandri MT, Colombo A, et al. Prognostic value of troponin I in cardiac risk stratification of cancer patients undergoing high-dose chemotherapy. Circulation. 2004;109(22):2749–2754. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
