

A Screening of Antineoplastic Drugs for Acute Myeloid Leukemia Reveals Contrasting Immunogenic Effects of Etoposide and Fludarabine
- PMID: 32948017
- PMCID: PMC7556041
- DOI: 10.3390/ijms21186802
A Screening of Antineoplastic Drugs for Acute Myeloid Leukemia Reveals Contrasting Immunogenic Effects of Etoposide and Fludarabine
Abstract
Background: Recent evidence demonstrated that the treatment of acute myeloid leukemia (AML) cells with daunorubicin (DNR) but not cytarabine (Ara-C) results in immunogenic cell death (ICD). In the clinical setting, chemotherapy including anthracyclines and Ara-C remains a gold standard for AML treatment. In the last decade, etoposide (Eto) and fludarabine (Flu) have been added to the standard treatment for AML to potentiate its therapeutic effect and have been tested in many trials. Very little data are available about the ability of these drugs to induce ICD.
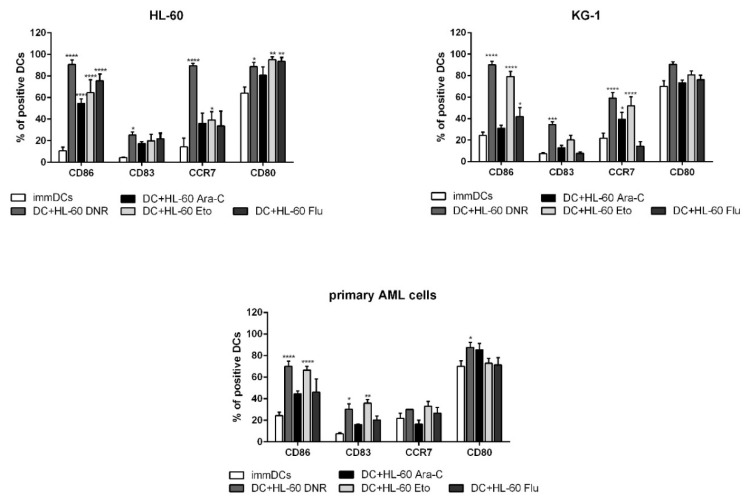
Methods: AML cells were treated with all four drugs. Calreticulin and heat shock protein 70/90 translocation, non-histone chromatin-binding protein high mobility group box 1 and adenosine triphosphate release were evaluated. The treated cells were pulsed into dendritic cells (DCs) and used for in vitro immunological tests.
Results: Flu and Ara-C had no capacity to induce ICD-related events. Interestingly, Eto was comparable to DNR in inducing all ICD events, resulting in DC maturation. Moreover, Flu was significantly more potent in inducing suppressive T regulatory cells compared to other drugs.
Conclusions: Our results indicate a novel and until now poorly investigated feature of antineoplastic drugs commonly used for AML treatment, based on their different immunogenic potential.
Keywords: acute myeloid leukemia; chemotherapy; etoposide; fludarabine; immunogenic cell death.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
-
- Lecciso M., Ocadlikova D., Sangaletti S., Trabanelli S., De Marchi E., Orioli E., Pegoraro A., Portararo P., Jandus C., Bontadini A., et al. ATP Release from Chemotherapy-Treated Dying Leukemia Cells Elicits an Immune Suppressive Effect by Increasing Regulatory T Cells and Tolerogenic Dendritic Cells. Front. Immunol. 2017;8:1918. doi: 10.3389/fimmu.2017.01918. - DOI - PMC - PubMed
-
- Fucikova J., Truxova I., Hensler M., Becht E., Kasikova L., Moserova I., Vosahlikova S., Klouckova J., Church S.E., Cremer I., et al. Calreticulin exposure by malignant blasts correlates with robust anticancer immunity and improved clinical outcome in AML patients. Blood. 2016;128:3113–3124. doi: 10.1182/blood-2016-08-731737. - DOI - PMC - PubMed
-
- Wemeau M., Kepp O., Tesnière A., Panaretakis T., Flament C., De Botton S., Zitvogel L., Kroemer G., Chaput N. Calreticulin exposure on malignant blasts predicts a cellular anticancer immune response in patients with acute myeloid leukemia. Cell Death Dis. 2010;1:e104. doi: 10.1038/cddis.2010.82. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
