

Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: Systematic Review and Meta-Analysis of Randomised Controlled Trials
- PMID: 32948060
- PMCID: PMC7559694
- DOI: 10.3390/antibiotics9090610
Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: Systematic Review and Meta-Analysis of Randomised Controlled Trials
Abstract
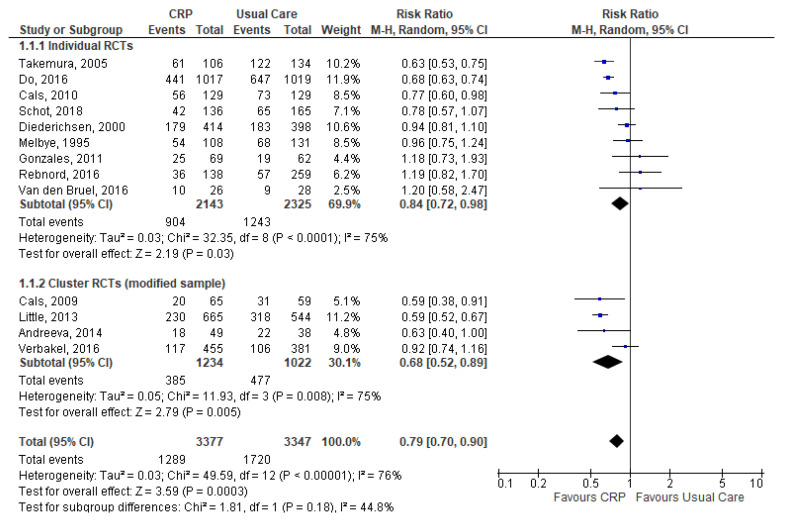
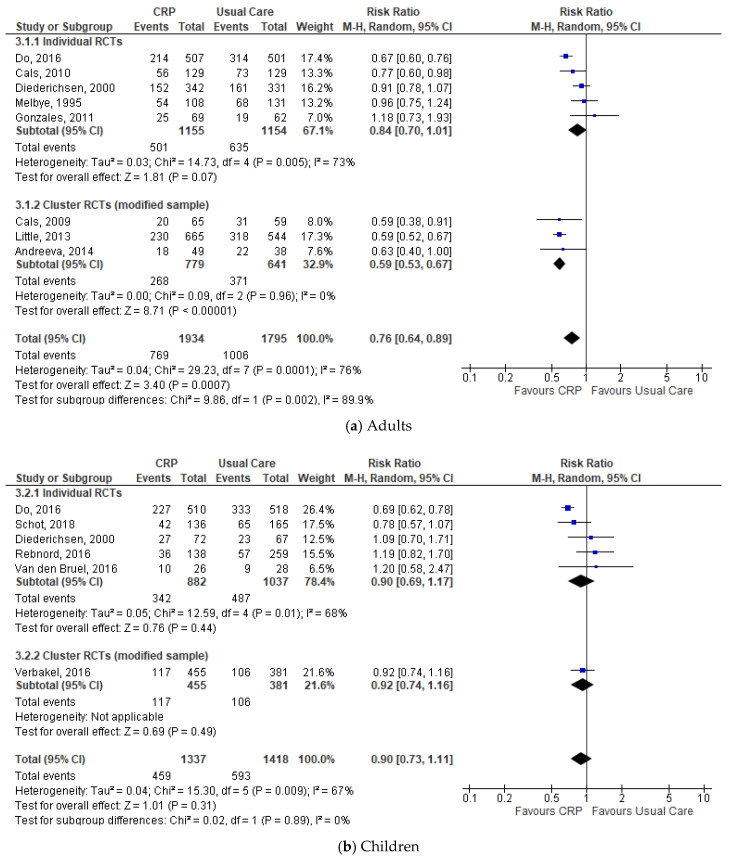
C-reactive protein (CRP) point-of-care testing (POCT) is increasingly being promoted to reduce diagnostic uncertainty and enhance antibiotic stewardship. In primary care, respiratory tract infections (RTIs) are the most common reason for inappropriate antibiotic prescribing, which is a major driver for antibiotic resistance. We systematically reviewed the available evidence on the impact of CRP-POCT on antibiotic prescribing for RTIs in primary care. Thirteen moderate to high-quality studies comprising 9844 participants met our inclusion criteria. Meta-analyses showed that CRP-POCT significantly reduced immediate antibiotic prescribing at the index consultation compared with usual care (RR 0.79, 95%CI 0.70 to 0.90, p = 0.0003, I2 = 76%) but not during 28-day (n = 7) follow-up. The immediate effect was sustained at 12 months (n = 1). In children, CRP-POCT reduced antibiotic prescribing when CRP (cut-off) guidance was provided (n = 2). Meta-analyses showed significantly higher rates of re-consultation within 30 days (n = 8, 1 significant). Clinical recovery, resolution of symptoms, and hospital admissions were not significantly different between CRP-POCT and usual care. CRP-POCT can reduce immediate antibiotic prescribing for RTIs in primary care (number needed to (NNT) for benefit = 8) at the expense of increased re-consultations (NNT for harm = 27). The increase in re-consultations and longer-term effects of CRP-POCT need further evaluation. Overall, the benefits of CRP-POCT outweigh the potential harms (NNTnet = 11).
Keywords: antibiotic prescribing; antibiotic stewardship; antibiotic use; c-reactive protein; diagnostics; meta-analysis; point-of-care testing; primary care; respiratory tract infection; systematic review.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Centers for Disease Control and Prevention Measuring Outpatient Antibiotic Prescribing. [(accessed on 10 June 2020)];2020 Available online: https://www.cdc.gov/antibiotic-use/community/programs-measurement/measur....
-
- Fleming-Dutra K.E., Hersh A.L., Shapiro D.J., Bartoces M., Enns E.A., File T.M., Jr., Finkelstein J.A., Gerber J.S., Hyun D.Y., Linder J.A., et al. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010–2011. JAMA. 2016;315:1864–1873. doi: 10.1001/jama.2016.4151. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
