

Successful management of zinc phosphide poisoning-a Hungarian case
- PMID: 32948124
- PMCID: PMC7501600
- DOI: 10.1186/s12245-020-00307-8
Successful management of zinc phosphide poisoning-a Hungarian case
Abstract
Background: Zinc phosphide (ZnP) is the basic component of several insecticides easily accessible worldwide. Intentional or accidental intoxication may lead to severe complications and multiple organ failure, resulting in high mortality. No known antidote is currently available. The iron-chelation and the antioxidative effects are well-known features of alpha-lipoic acid (ALA), although its use in the treatment of ZnP poisoning has not been documented previously. We describe the case of a patient with serious ZnP poisoning with multiple organ failure, where ALA was also included in the patient's supportive therapy.
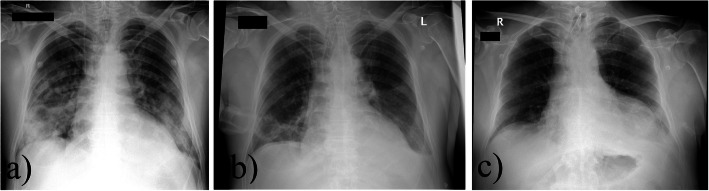
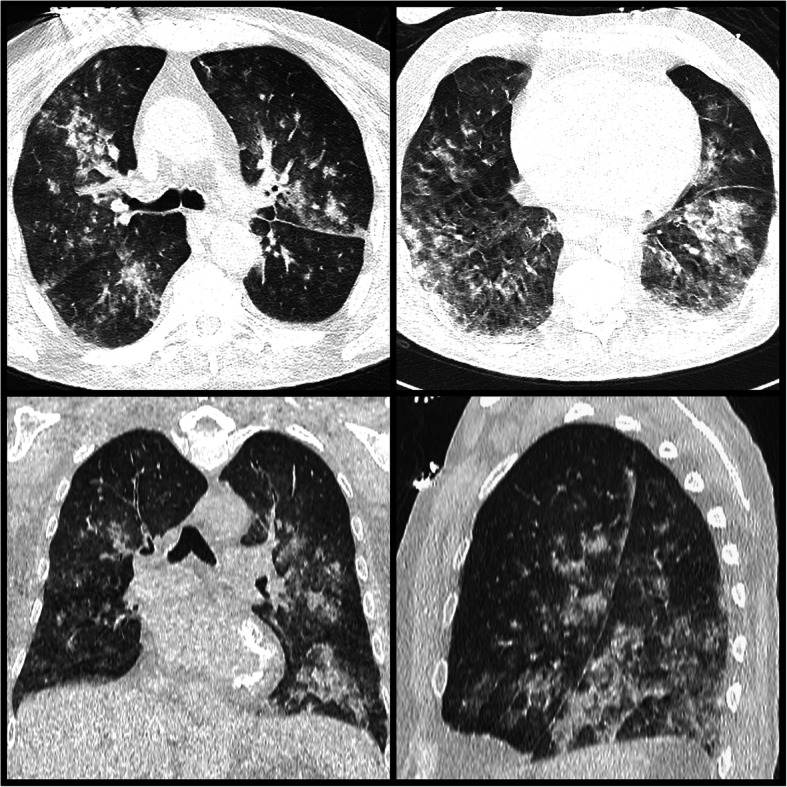
Case presentation: A 65-year-old man ingested 125 g of Arvalin® (containing 5 g ZnP) and presented to the Emergency Department, with respiratory insufficiency and decreased consciousness. He developed hypokalemia, hypocalcemia, low white blood cell count, elevated C-reactive protein level, mixed acidosis, hepatic and kidney damage, thickening of the jejunal wall, and lung atelectasis, which served as a basis for the ensuing bacterial pneumonia. Antibiotics and adequate supportive therapy were provided. Laboratory tests indicated liver damage (slightly increased liver enzymes, low pseudocholinesterase levels; 706 U/L on day 2), possibly caused by the patient's chronic alcoholism or the ZnP poison itself, therefore, hepatoprotective agents, ALA (Thiogamma Turbo-Set®) with N-acetylcysteine were administered for six consecutive days. Pseudocholinesterase values increased sixfold until the end of the second week of care. Fifteen days after admission, the patient was relocated to the department of psychiatry with stable vital functions, clear consciousness, declining inflammatory markers, and improved liver function. He was discharged 1 month later, fully recovered.
Conclusions: Our case is the first documented voluntary and severe ZnP poisoning in Hungary. Our patient developed multiple organ failure and atelectasis, possibly resulting in the observed respiratory infection. The development of bacterial pneumonia highlighted the dangers of phosphine-induced atelectasis. The use of ALA in our patient's case, as an antioxidant and agent for metal chelation, suggested that this agent could be a promising tool in the prevention and treatment of ZnP-induced hepatic damage.
Keywords: Alpha-lipoic acid; Dihydrolipoic acid; N-acetylcysteine; Pneumonia; Poisoning; Pseudocholinesterase; Zinc phosphide.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Successful Management of Aluminium Phosphide Poisoning Resulting in Cardiac Arrest.Turk J Anaesthesiol Reanim. 2015 Aug;43(4):288-90. doi: 10.5152/TJAR.2015.75010. Epub 2015 Mar 3. Turk J Anaesthesiol Reanim. 2015. PMID: 27366514 Free PMC article.
-
A case report of zinc phosphide poisoning: complicated by acute renal failure and tubulo interstitial nephritis.BMC Pharmacol Toxicol. 2017 May 25;18(1):37. doi: 10.1186/s40360-017-0144-7. BMC Pharmacol Toxicol. 2017. PMID: 28545504 Free PMC article.
-
Hepatotoxicity due to zinc phosphide poisoning in two patients: role of N-acetylcysteine.Clin Case Rep. 2016 Jul 6;4(8):768-72. doi: 10.1002/ccr3.618. eCollection 2016 Aug. Clin Case Rep. 2016. PMID: 27525081 Free PMC article.
-
Aluminium and zinc phosphide poisoning.Clin Toxicol (Phila). 2009 Feb;47(2):89-100. doi: 10.1080/15563650802520675. Clin Toxicol (Phila). 2009. PMID: 19280425 Review.
-
Zinc Phosphide Poisoning: From A to Z.Toxics. 2023 Jun 25;11(7):555. doi: 10.3390/toxics11070555. Toxics. 2023. PMID: 37505522 Free PMC article. Review.
Cited by
-
The role of alcohol use in pesticide suicide and self-harm: a scoping review.Soc Psychiatry Psychiatr Epidemiol. 2024 Feb;59(2):211-232. doi: 10.1007/s00127-023-02526-9. Epub 2023 Jul 8. Soc Psychiatry Psychiatr Epidemiol. 2024. PMID: 37420003 Free PMC article.
-
Toxicoepidemiology of Phosphide Poisoning in the Central Part of Iran.J Res Pharm Pract. 2023 Nov 27;12(1):21-28. doi: 10.4103/jrpp.jrpp_20_23. eCollection 2023 Jan-Mar. J Res Pharm Pract. 2023. PMID: 38213604 Free PMC article.
-
In vivo treatment of zinc phosphide poisoning by administration of mesoporous silica nanoparticles as an effective antidote agent.Heliyon. 2024 Apr 16;10(8):e29458. doi: 10.1016/j.heliyon.2024.e29458. eCollection 2024 Apr 30. Heliyon. 2024. PMID: 38681564 Free PMC article.
-
Outcome of Rodenticide Poisoning and Its Associated Factors Among Adult Patients Admitted with Rodenticide Poisoning at the Emergency Unit of Debre Tabor Comprehensive Specialized Hospital, Debre Tabor, North Central Ethiopia.Open Access Emerg Med. 2023 May 26;15:189-197. doi: 10.2147/OAEM.S405970. eCollection 2023. Open Access Emerg Med. 2023. PMID: 37260736 Free PMC article.
-
A case report on zinc phosphide ingestion resulting to acute pancreatitis.Ann Med Surg (Lond). 2022 May 24;78:103859. doi: 10.1016/j.amsu.2022.103859. eCollection 2022 Jun. Ann Med Surg (Lond). 2022. PMID: 35734667 Free PMC article.
References
-
- Chugh SN. Aluminium phosphide poisoning: present status and management. J Assoc Physicians India. 1992;40(6):401–405. - PubMed
-
- Chefurka W, Kashi KP, Bond EJ. The effect of phosphine on electron transport in mitochondria. Pestic Biochem Physiol. 1976;6(1):65–84. doi: 10.1016/0048-3575(76)90010-9. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
