

Membranous nephropathy in patients with HIV: a report of 11 cases
- PMID: 32948130
- PMCID: PMC7501617
- DOI: 10.1186/s12882-020-02042-x
Membranous nephropathy in patients with HIV: a report of 11 cases
Abstract
Background: Membranous nephropathy (MN) has been recognized to occur in patients with human immunodeficiency virus (HIV) infection since the beginning of the HIV epidemic. The prevalence of phospholipase A2 receptor (PLA2R)-associated MN in this group has not been well studied.
Methods: We conducted a retrospective review of electronic pathology databases at three institutions to identify patients with MN and known HIV at the time of renal biopsy. Patients with comorbidities and coinfections known to be independently associated with MN were excluded.
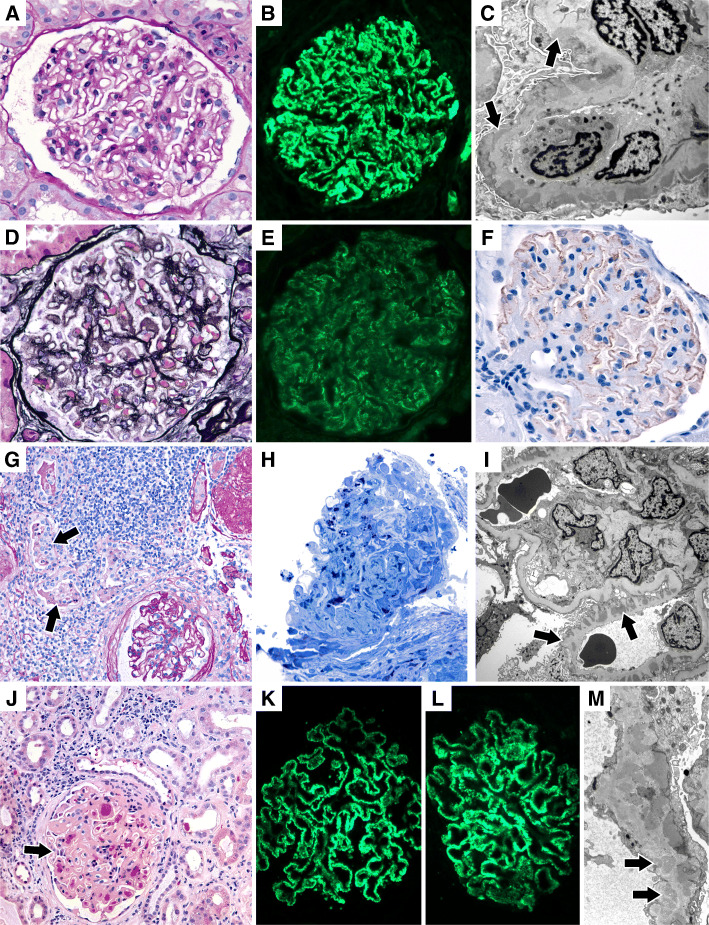
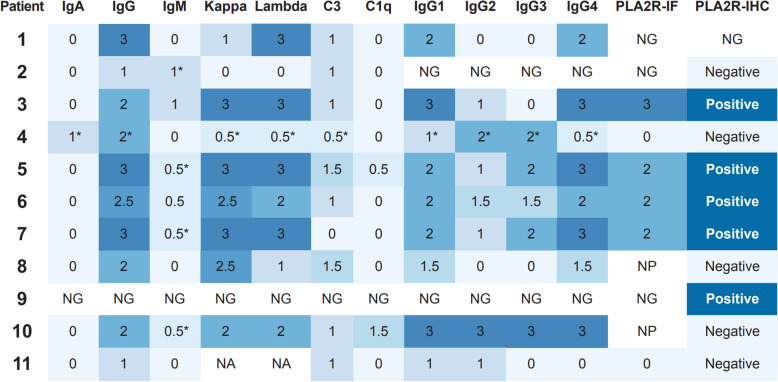
Results: We identified 11 HIV-positive patients with biopsy-confirmed MN meeting inclusion and exclusion criteria. Patient ages ranged from 39 to 66 years old, and 10 of 11 patients (91%) were male. The majority of patients presented with nephrotic-range proteinuria, were on anti-retroviral therapy at the time of biopsy and had low or undetectable HIV viral loads. Biopsies from 5 of 10 (50%) patients demonstrated capillary wall staining for PLA2R. Measurement of serum anti-PLA2R antibodies was performed in three patients, one of whom had positive anti-PLA2R antibody titers. Follow-up data was available on 10 of 11 patients (median length of follow-up: 44 months; range: 4-145 months). All patients were maintained on anti-retroviral therapy (ARV) and 5 patients (52%) received concomitant immunosuppressive regimens. Three patients developed end-stage renal disease (ESRD) during the follow-up period.
Conclusions: MN in the setting of HIV is often identified in the setting of an undetectable viral loads, and similar to other chronic viral infection-associated MNs, ~ 50% of cases demonstrate tissue reactivity with PLA2R antigen, which may be seen without corresponding anti-PLA2R serum antibodies.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
PLA2R antibodies and PLA2R glomerular deposits in psoriasis patients with membranous nephropathy.BMC Nephrol. 2016 Nov 22;17(1):185. doi: 10.1186/s12882-016-0407-3. BMC Nephrol. 2016. PMID: 27876003 Free PMC article.
-
Renal phospholipase A2 receptor in hepatitis B virus-associated membranous nephropathy.Am J Nephrol. 2015;41(4-5):345-53. doi: 10.1159/000431331. Epub 2015 Jun 13. Am J Nephrol. 2015. PMID: 26087695
-
Autoantibodies against phospholipase A2 receptor in Korean patients with membranous nephropathy.PLoS One. 2013 Apr 26;8(4):e62151. doi: 10.1371/journal.pone.0062151. Print 2013. PLoS One. 2013. PMID: 23637987 Free PMC article.
-
Sjögren's syndrome complicated with membranous nephropathy, a cause or coincidence?Int J Rheum Dis. 2021 Aug;24(8):1086-1094. doi: 10.1111/1756-185X.14168. Epub 2021 Jul 5. Int J Rheum Dis. 2021. PMID: 34223708 Review.
-
[Anti-NEP and anti-PLA2R antibodies in membranous nephropathy: an update].Rev Med Brux. 2015 May-Jun;36(3):166-71. Rev Med Brux. 2015. PMID: 26372979 Review. French.
Cited by
-
Human Immunodeficiency Virus-associated Immune Complex Kidney Disease Progressing to End-stage Kidney Disease.Intern Med. 2023 Nov 1;62(21):3183-3186. doi: 10.2169/internalmedicine.1415-22. Epub 2023 Mar 15. Intern Med. 2023. PMID: 36927969 Free PMC article.
-
Autoimmunity and Infection in Glomerular Disease.Microorganisms. 2023 Sep 2;11(9):2227. doi: 10.3390/microorganisms11092227. Microorganisms. 2023. PMID: 37764071 Free PMC article. Review.
-
Viral Infection Associated Membranous Nephropathy: Clinical Presentation and Outcomes.Indian J Nephrol. 2025 Jan-Feb;35(1):70-76. doi: 10.25259/IJN_57_2024. Epub 2024 Aug 1. Indian J Nephrol. 2025. PMID: 39872252 Free PMC article.
-
NELL1 membranous nephropathy: clinical associations provide mechanistic clues.Front Nephrol. 2024 Mar 26;4:1323432. doi: 10.3389/fneph.2024.1323432. eCollection 2024. Front Nephrol. 2024. PMID: 38596642 Free PMC article. Review.
-
NELL1-Positive HIV-Associated Lupus-Like Membranous Nephropathy with Spontaneous Remission.Glomerular Dis. 2022 Jun 29;2(4):184-188. doi: 10.1159/000525541. eCollection 2022. Glomerular Dis. 2022. PMID: 36817287 Free PMC article.
References
-
- Hou J, Nast CC. Changing concepts of HIV infection and renal disease. Curr Opin Nephrol Hypertens 2018;27:144–152. https://doi.org/10.1097/MNH.0000000000000400. - PubMed
-
- Kupin WL. Viral-Associated GN: Hepatitis C and HIV. Clin J Am Soc Nephrol 2017;12:1337–1342. https://doi.org/10.2215/CJN.04320416. - PMC - PubMed
-
- Haas M, Kaul S, Eustace JA. HIV-associated immune complex glomerulonephritis with “lupus-like” features: a clinicopathologic study of 14 cases. Kidney Int 2005;67:1381–1390. https://doi.org/10.1111/j.1523-1755.2005.00215.x. - PubMed
-
- Foy MC, Estrella MM, Lucas GM, Tahir F, Fine DM, Moore RD, et al. Comparison of risk factors and outcomes in HIV immune complex kidney disease and HIV-associated nephropathy. Clin J Am Soc Nephrol 2013;8:1524–1532. https://doi.org/10.2215/CJN.10991012. - PMC - PubMed
