

Total resection of a giant retroperitoneal and mediastinal ganglioneuroma-case report and systematic review of the literature
- PMID: 32948207
- PMCID: PMC7501651
- DOI: 10.1186/s12957-020-02016-1
Total resection of a giant retroperitoneal and mediastinal ganglioneuroma-case report and systematic review of the literature
Abstract
Background: Ganglioneuromas (GNs) are extremely rare, slowly growing, benign tumors that can arise from Schwann cells, ganglion cells, and neuronal or fibrous tissues. Due to their origin from the sympathetic neural crest, they show neuroendocrine potential; however, most are reported to be hormonally inactive. Nevertheless, complete surgical removal is recommended for symptom control or for the prevention of potential malignant degeneration.
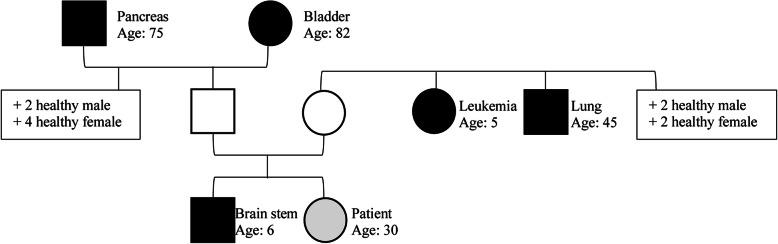
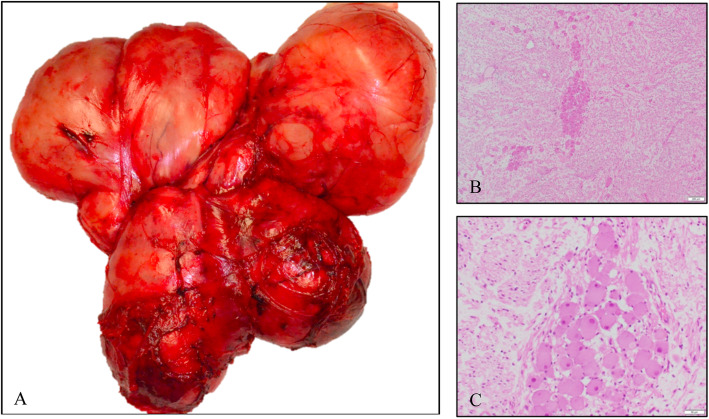
Case report: A 30-year-old female was referred to our oncologic center due to a giant retroperitoneal and mediastinal mass detected in computed tomography (CT) scans. The initial symptoms were transient nausea, diarrhea, and crampy abdominal pain. There was a positive family history including 5 first- and second-degree relatives. Presurgical biopsy revealed a benign ganglioneuroma. Total resection (TR) of a 35 × 25 × 25 cm, 2550-g tumor was obtained successfully via laparotomy combined with thoracotomy and partial incision of the diaphragm. Histopathological analysis confirmed the diagnosis. Surgically challenging aspects were the bilateral tumor invasion from the retroperitoneum into the mediastinum through the aortic hiatus with the need of a bilateral 2-cavity procedure, as well as the tumor-related displacement of the abdominal aorta, the mesenteric vessels, and the inferior vena cava. Due to their anatomic course through the tumor mass, the lumbar aortic vessels needed to be partially resected. Postoperative functioning was excellent without any sign of neurologic deficit.
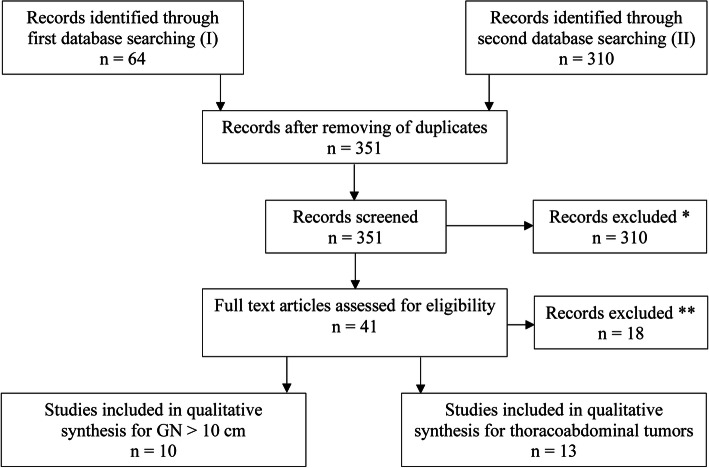
Conclusion: Here, we present the largest case of a TR of a GN with retroperitoneal and mediastinal expansion. On review of the literature, this is the largest reported GN resected and was performed safely. Additionally, we present the first systematic literature review for large GN (> 10 cm) as well as for resected tumors growing from the abdominal cavity into the thoracic cavity.
Keywords: Case report; Ganglioneuroma; Largest; Systematic review; Thoracoabdominal.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
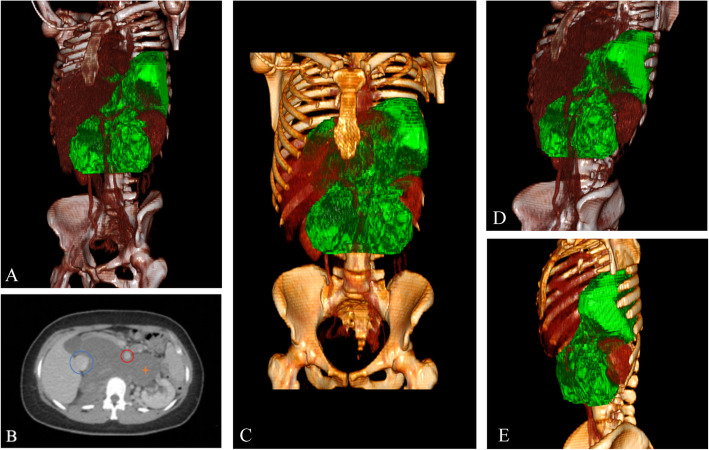
 , aorta
, aorta  , tumor
, tumor 
Similar articles
-
Retroperitoneal paravertebral ganglioneuroma: a multidisciplinary approach facilitates less radical surgery.World J Surg Oncol. 2016 Jul 26;14(1):194. doi: 10.1186/s12957-016-0953-y. World J Surg Oncol. 2016. PMID: 27461001 Free PMC article.
-
Large Asymptomatic Retroperitoneal Ganglioneuroma Displacing Major Abdominal Organs and Vessels in an Adult.Am J Case Rep. 2021 Jun 22;22:e931725. doi: 10.12659/AJCR.931725. Am J Case Rep. 2021. PMID: 34155189 Free PMC article.
-
Ganglioneuroma presenting as an asymptomatic huge posterior mediastinal and retroperitoneal tumor.J Chin Med Assoc. 2003 Jun;66(6):370-4. J Chin Med Assoc. 2003. PMID: 12889507
-
Retroperitoneal ganglioneuroma with nodal involvement in an adult patient with human immunodeficiency virus: a case report and review of the literature.J Med Case Rep. 2021 Dec 28;15(1):634. doi: 10.1186/s13256-021-03134-4. J Med Case Rep. 2021. PMID: 34963492 Free PMC article. Review.
-
Idiopathic aneurysm of inferior vena cava associated with retroperitoneal ganglioneuroma: case report.J Vasc Surg. 2003 Apr;37(4):895-8. doi: 10.1067/mva.2003.172. J Vasc Surg. 2003. PMID: 12663996 Review.
Cited by
-
A case report of multimodal ultrasound imaging in the diagnosis of giant retroperitoneal ganglioneuroma.Cancer Innov. 2023 May 10;2(5):433-437. doi: 10.1002/cai2.73. eCollection 2023 Oct. Cancer Innov. 2023. PMID: 38090383 Free PMC article.
-
Retroperitoneal ganglioneuroma presenting as an obstructive pyelonephritis: a case report.J Surg Case Rep. 2021 Apr 24;2021(4):rjab104. doi: 10.1093/jscr/rjab104. eCollection 2021 Apr. J Surg Case Rep. 2021. PMID: 33927851 Free PMC article.
-
Overreliance on Radiological Findings Leading to Misdiagnosed Giant Retroperitoneal Ganglioneuroma: A Case Report and Literature Review.Cureus. 2023 Aug 22;15(8):e43914. doi: 10.7759/cureus.43914. eCollection 2023 Aug. Cureus. 2023. PMID: 37746449 Free PMC article.
-
Imaging of Ganglioneuroma: A Literature Review and a Rare Case of Cystic Presentation in an Adolescent Girl.Diagnostics (Basel). 2023 Jun 27;13(13):2190. doi: 10.3390/diagnostics13132190. Diagnostics (Basel). 2023. PMID: 37443583 Free PMC article.
-
Combined exploratory laparotomy, transpsoas, and thoracic approach to resection of a giant spinal ganglioneuroma: illustrative case.J Neurosurg Case Lessons. 2023 Jan 9;5(2):CASE22453. doi: 10.3171/CASE22453. Print 2023 Jan 9. J Neurosurg Case Lessons. 2023. PMID: 36624632 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
