

Acute Kidney Injury and Risk of CKD and Hypertension after Pediatric Cardiac Surgery
- PMID: 32948644
- PMCID: PMC7536759
- DOI: 10.2215/CJN.00150120
Acute Kidney Injury and Risk of CKD and Hypertension after Pediatric Cardiac Surgery
Abstract
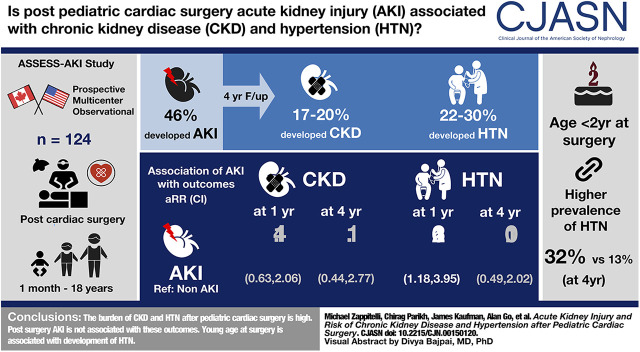
Background and objectives: The association of AKI after pediatric cardiac surgery with long-term CKD and hypertension development is unclear. The study objectives were to determine whether AKI after pediatric cardiac surgery is associated with incident CKD and hypertension.
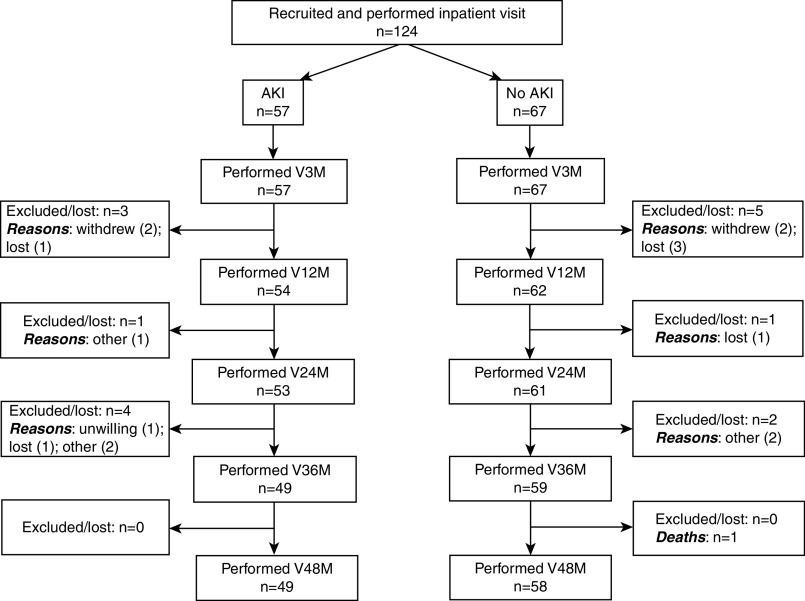
Design, setting, participants, & measurements: This was a prospective cohort study of children of 1 month to 18 years old who were undergoing cardiac surgery at two tertiary care centers (Canada, United States). Participants were recruited before cardiac surgery and were followed during hospitalization and at 3, 12, 24, 36, and 48 months after discharge. Exposures were postoperative AKI, based on the Kidney Disease Improving Global Outcomes (KDIGO) definition, and age <2 years old at surgery. Outcomes and measures were CKD (low eGFR or albuminuria for age) and hypertension (per the 2017 American Academy of Pediatrics guidelines) at follow-up, with the composite outcome of CKD or hypertension.
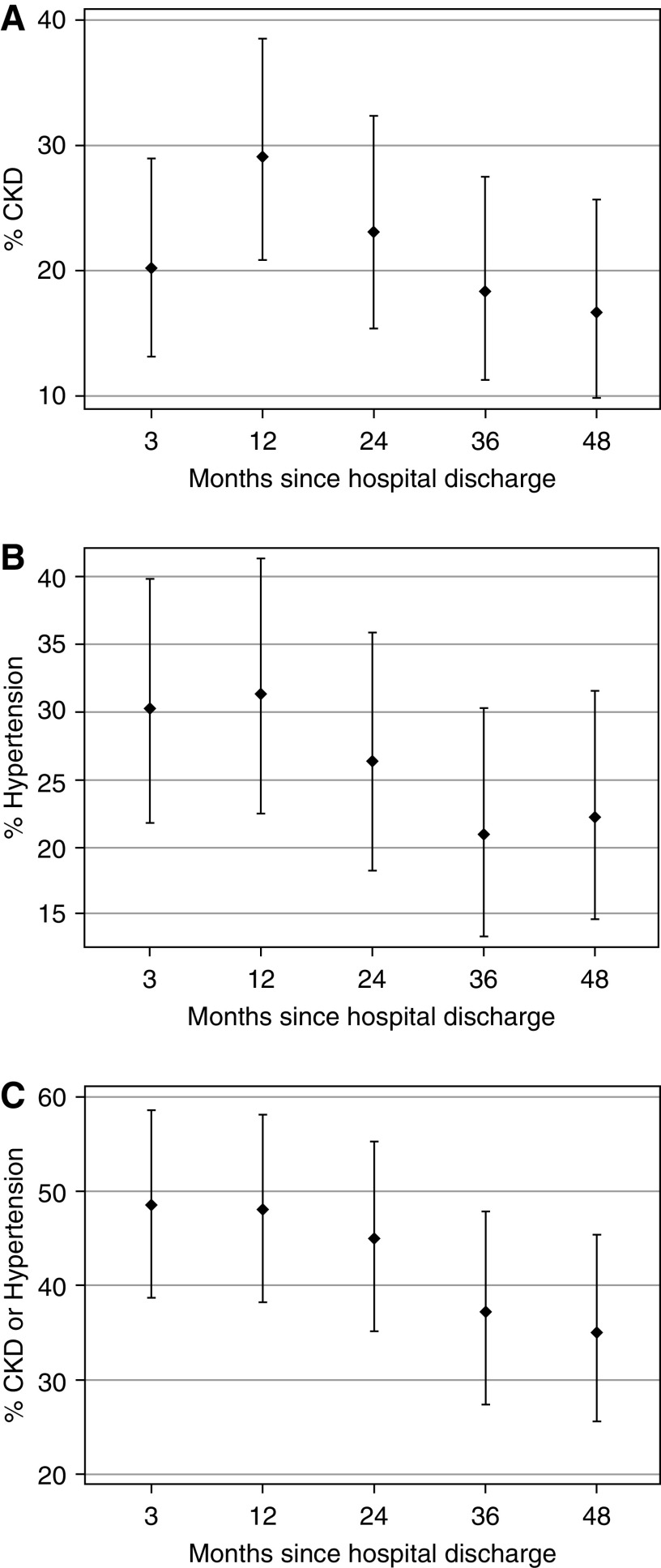
Results: Among 124 participants, 57 (46%) developed AKI. AKI versus non-AKI participants had a median (interquartile range) age of 8 (4.8-40.8) versus 46 (6.0-158.4) months, respectively, and higher preoperative eGFR. From the 3- to 48-month follow-up, the cohort prevalence of CKD was high (17%-20%); hypertension prevalence was also high (22%-30%). AKI was not significantly associated with the development of CKD throughout follow-up. AKI was associated with hypertension development at 12 months after discharge (adjusted relative risk, 2.16; 95% confidence interval, 1.18 to 3.95), but not at subsequent visits. Children aged <2 years old at surgery had a significantly higher prevalence of hypertension during follow-up than older children (40% versus 21% at 3-month follow-up; 32% versus 13% at 48-month follow-up).
Conclusions: CKD and hypertension burden in the 4 years after pediatric cardiac surgery is high. Young age at surgery, but not AKI, is associated with their development.
Keywords: acute kidney injury; acute renal failure; chronic kidney disease; clinical hypertension; epidemiology and outcomes; pediatric intensive care medicine; pediatric nephrology.
Copyright © 2020 by the American Society of Nephrology.
Figures
References
-
- Alkandari O, Eddington KA, Hyder A, Gauvin F, Ducruet T, Gottesman R, Phan V, Zappitelli M: Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: A two-center retrospective cohort study. Crit Care 15: R146, 2011. - PMC - PubMed
-
- Zappitelli M, Bernier PL, Saczkowski RS, Tchervenkov CI, Gottesman R, Dancea A, Hyder A, Alkandari O: A small post-operative rise in serum creatinine predicts acute kidney injury in children undergoing cardiac surgery. Kidney Int 76: 885–892, 2009. - PubMed
-
- Zappitelli M, Krawczeski CD, Devarajan P, Wang Z, Sint K, Thiessen-Philbrook H, Li S, Bennett MR, Ma Q, Shlipak MG, Garg AX, Parikh CR; TRIBE-AKI Consortium : Early postoperative serum cystatin C predicts severe acute kidney injury following pediatric cardiac surgery. Kidney Int 80: 655–662, 2011. - PMC - PubMed
-
- Hirano D, Ito A, Yamada A, Kakegawa D, Miwa S, Umeda C, Chiba K, Takemasa Y, Tokunaga A, Ida H: Independent risk factors and 2-year outcomes of acute kidney injury after surgery for congenital heart disease. Am J Nephrol 46: 204–209, 2017. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
