Dissecting clinical heterogeneity of bipolar disorder using multiple polygenic risk scores
- PMID: 32948743
- PMCID: PMC7501305
- DOI: 10.1038/s41398-020-00996-y
Dissecting clinical heterogeneity of bipolar disorder using multiple polygenic risk scores
Abstract
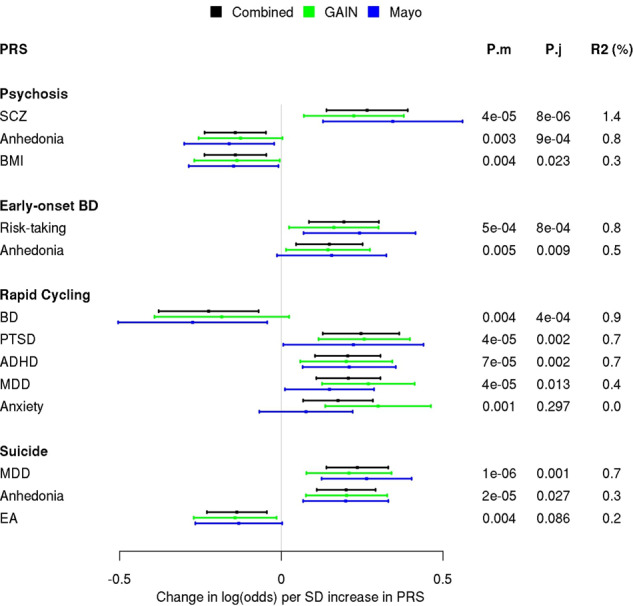
Bipolar disorder (BD) has high clinical heterogeneity, frequent psychiatric comorbidities, and elevated suicide risk. To determine genetic differences between common clinical sub-phenotypes of BD, we performed a systematic polygenic risk score (PRS) analysis using multiple PRSs from a range of psychiatric, personality, and lifestyle traits to dissect differences in BD sub-phenotypes in two BD cohorts: the Mayo Clinic BD Biobank (N = 968) and Genetic Association Information Network (N = 1001). Participants were assessed for history of psychosis, early-onset BD, rapid cycling (defined as four or more episodes in a year), and suicide attempts using questionnaires and the Structured Clinical Interview for DSM-IV. In a combined sample of 1969 bipolar cases (45.5% male), those with psychosis had higher PRS for SCZ (OR = 1.3 per S.D.; p = 3e-5) but lower PRSs for anhedonia (OR = 0.87; p = 0.003) and BMI (OR = 0.87; p = 0.003). Rapid cycling cases had higher PRS for ADHD (OR = 1.23; p = 7e-5) and MDD (OR = 1.23; p = 4e-5) and lower BD PRS (OR = 0.8; p = 0.004). Cases with a suicide attempt had higher PRS for MDD (OR = 1.26; p = 1e-6) and anhedonia (OR = 1.22; p = 2e-5) as well as lower PRS for educational attainment (OR = 0.87; p = 0.003). The observed novel PRS associations with sub-phenotypes align with clinical observations such as rapid cycling BD patients having a greater lifetime prevalence of ADHD. Our findings confirm that genetic heterogeneity contributes to clinical heterogeneity of BD and consideration of genetic contribution to psychopathologic components of psychiatric disorders may improve genetic prediction of complex psychiatric disorders.
Conflict of interest statement
Dr. Frye has received grant support from Assurex Health, Myriad, Pfizer, National Institute of Mental Health (RO1 MH079261), National Institute of Alcohol Abuse and Alcoholism (P20AA017830), and Mayo Foundation; has been a consultant to Janssen Global Services, LLC, Mitsubishi Tanabe Pharma Corporation, Myriad, Sunovion, and Teva Pharmaceuticals; has received CME/Travel Support/presentation from CME Outfitters Inc. and Sunovian; Mayo Clinic has a financial interest in AssureRx and OneOme. Dr. McElroy is a consultant to or member of the scientific advisory boards of Bracket, MedAvante, Naurex, Shire, and Sunovion. She is a principal or co-investigator on studies sponsored by the Agency for Healthcare Research & Quality (AHRQ), AstraZeneca, Cephalon, Forest, Marriott Foundation, National Institute of Mental Health, Orexigen Therapeutics, Inc., Shire, and Takeda Pharmaceutical Company Ltd. She is also an inventor on United States Patent No. 6,323,236 B2, Use of Sulfamate Derivatives for Treating Impulse Control Disorders, and along with the patent’s assignee, University of Cincinnati, Cincinnati, Ohio, has received payments from Johnson & Johnson, which has exclusive rights under the patent. In the last 3 years, Dr Weissman has received research funds from NIMH, Templeton Foundation, Brain and Behavior and the Sackler Foundation, and has received royalties for publications of books on interpersonal psychotherapy from Perseus Press, Oxford University Press, on other topics from the American Psychiatric Association Press and royalties on the social adjustment scale from Multihealth Systems. None of these represent a conflict of interest.
Figures