

Ampakines stimulate phrenic motor output after cervical spinal cord injury
- PMID: 32949571
- PMCID: PMC8785412
- DOI: 10.1016/j.expneurol.2020.113465
Ampakines stimulate phrenic motor output after cervical spinal cord injury
Abstract
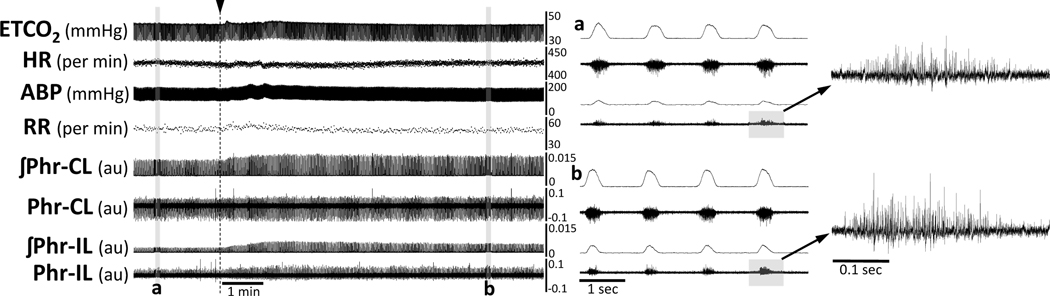
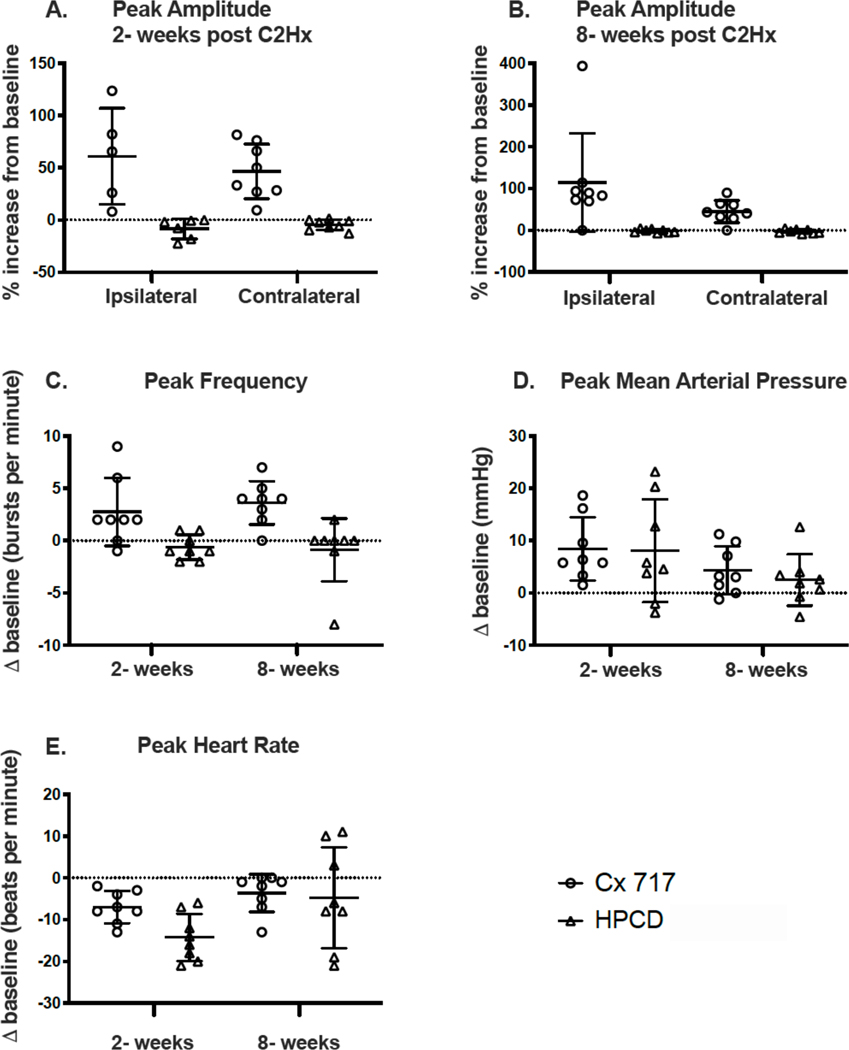
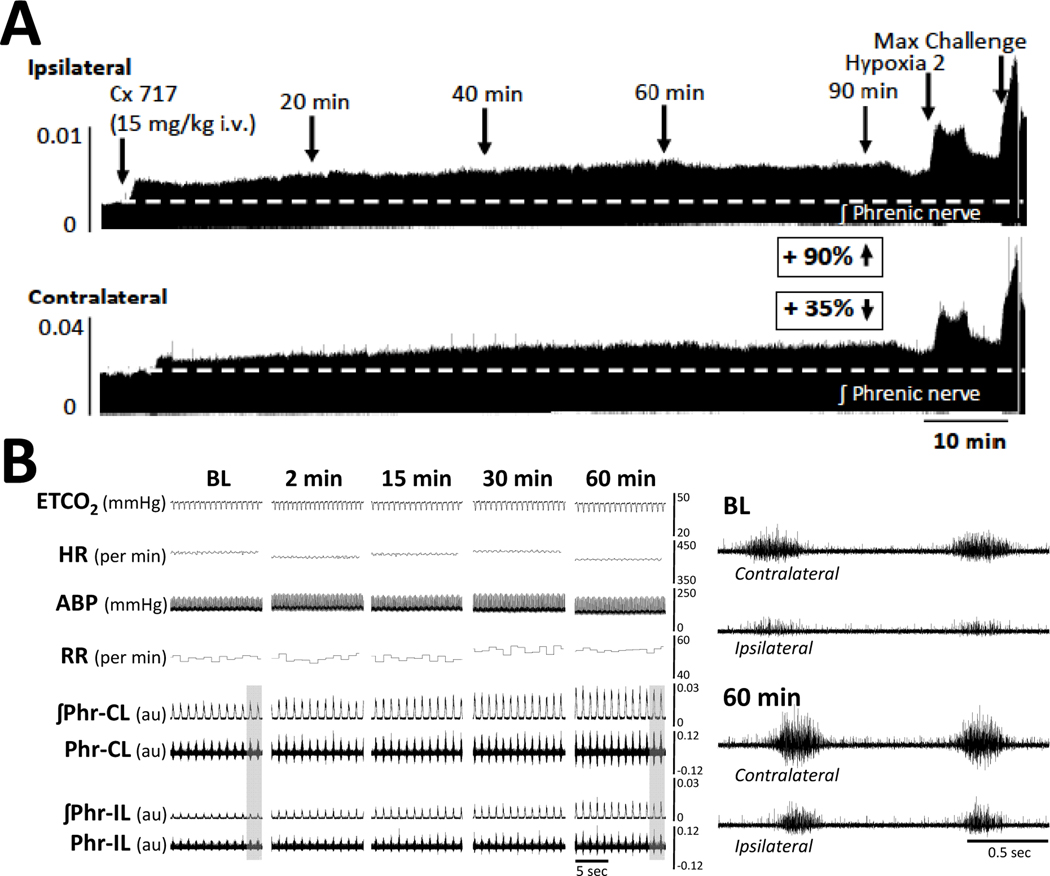
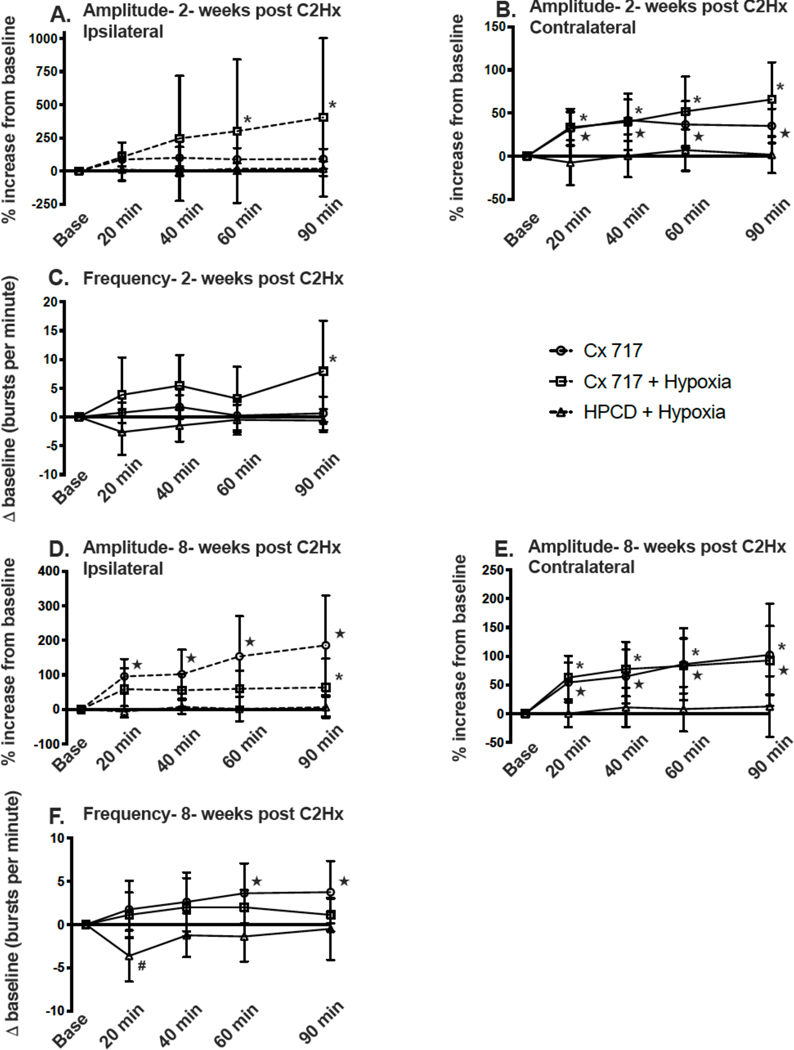
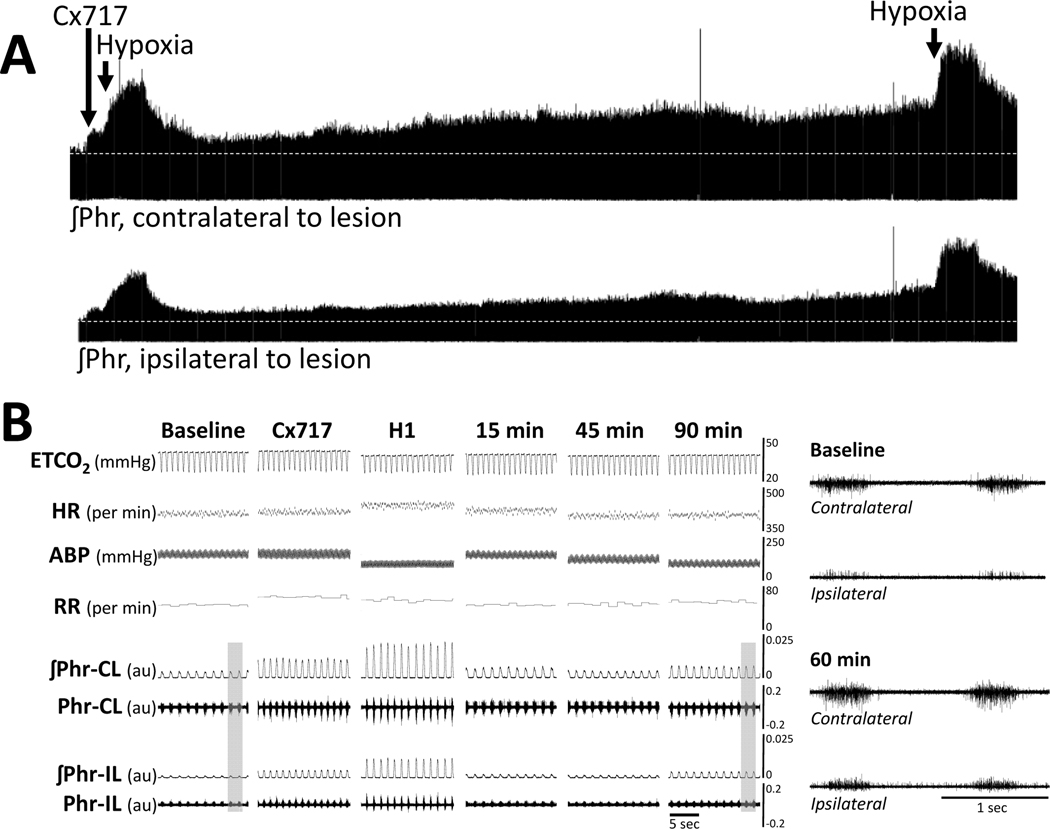
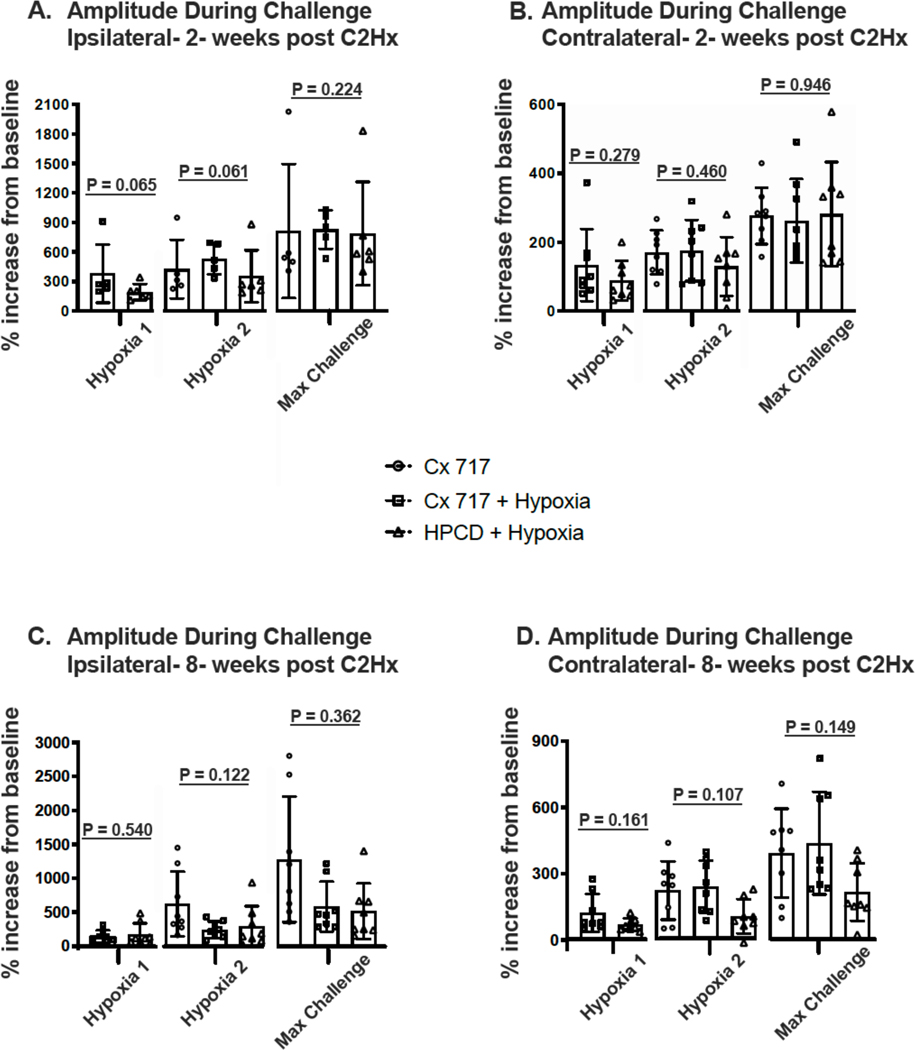
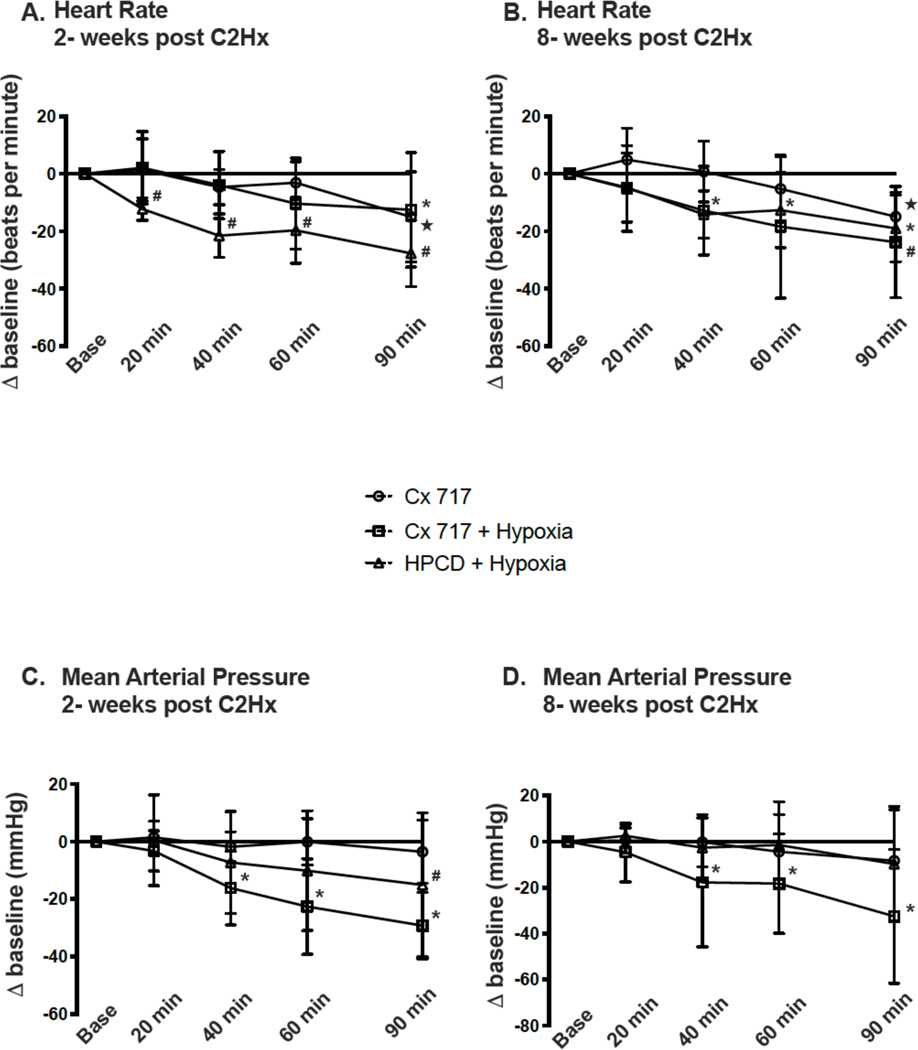
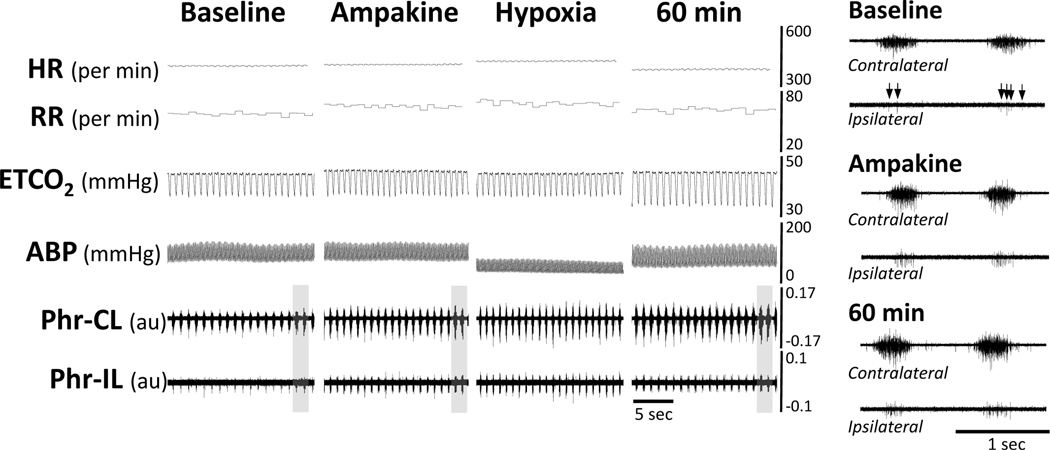
Activation of α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptors increases phrenic motor output. Ampakines are a class of drugs that are positive allosteric modulators of AMPA receptors. We hypothesized that 1) ampakines can stimulate phrenic activity after incomplete cervical spinal cord injury (SCI), and 2) pairing ampakines with brief hypoxia could enable sustained facilitation of phrenic bursting. Phrenic activity was recorded ipsilateral (IL) and contralateral (CL) to C2 spinal cord hemisection (C2Hx) in anesthetized adult rats. Two weeks after C2Hx, ampakine CX717 (15 mg/kg, i.v.) increased IL (61 ± 46% baseline, BL) and CL burst amplitude (47 ± 26%BL) in 8 of 8 rats. After 90 min, IL and CL bursting remained above baseline (BL) in 7 of 8 rats. Pairing ampakine with a single bout of acute hypoxia (5-min, arterial partial pressure of O2 ~ 50 mmHg) had a variable impact on phrenic bursting, with some rats showing a large facilitation that exceeded the response of the ampakine alone group. At 8 weeks post-C2Hx, 7 of 8 rats increased IL (115 ± 117%BL) and CL burst amplitude (45 ± 27%BL) after ampakine. The IL burst amplitude remained above BL for 90-min in 7 of 8 rats; CL bursting remained elevated in 6 of 8 rats. The sustained impact of ampakine at 8 weeks was not enhanced by hypoxia exposure. Intravenous vehicle (10% 2-Hydroxypropyl-β-cyclodextrin) did not increase phrenic bursting at either time point. We conclude that ampakines effectively stimulate neural drive to the diaphragm after cervical SCI. Pairing ampakines with a single hypoxic exposure did not consistently enhance phrenic motor facilitation.
Keywords: Ampakine; Hypoxia; Neuroplasticity; Phrenic; Respiratory; Spinal cord injury.
Copyright © 2020. Published by Elsevier Inc.
Figures
References
-
- Alilain WJ, Goshgarian HG, 2008. Glutamate receptor plasticity and activity-regulated cytoskeletal associated protein regulation in the phrenic motor nucleus may mediate spontaneous recovery of the hemidiaphragm following chronic cervical spinal cord injury. Experimental neurology 212, 348–357. - PMC - PubMed
-
- Arai A, Kessler M, Rogers G, Lynch G, 1996. Effects of a memory-enhancing drug on DL-alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor currents and synaptic transmission in hippocampus. The Journal of pharmacology and experimental therapeutics 278, 627–638. - PubMed
-
- Arai AC, Kessler M, 2007. Pharmacology of ampakine modulators: from AMPA receptors to synapses and behavior. Current drug targets 8, 583–602. - PubMed
-
- Arai AC, Xia YF, Rogers G, Lynch G, Kessler M, 2002. Benzamide-type AMPA receptor modulators form two subfamilies with distinct modes of action. The Journal of pharmacology and experimental therapeutics 303, 1075–1085. - PubMed
-
- Arai AC, Xia YF, Suzuki E, 2004. Modulation of AMPA receptor kinetics differentially influences synaptic plasticity in the hippocampus. Neuroscience 123, 1011–1024. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
