

The Clinical Role of Preoperative Serum CA19-9 and Carcinoembryonic Antigen (CEA) Levels in Evaluating the Resectability of Advanced Gallbladder Cancer
- PMID: 32950997
- PMCID: PMC7513615
- DOI: 10.12659/MSM.925017
The Clinical Role of Preoperative Serum CA19-9 and Carcinoembryonic Antigen (CEA) Levels in Evaluating the Resectability of Advanced Gallbladder Cancer
Abstract
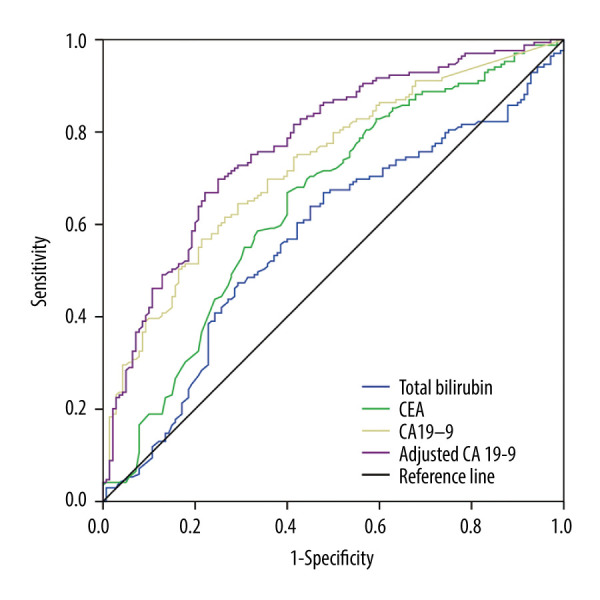
BACKGROUND The present study was designed to study the ability of preoperative serum concentrations of the tumor-associated biomarkers carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9) and adjusted CA19-9 to assess the resectability of advanced gallbladder cancer (GBC). MATERIAL AND METHODS This retrospective study included patients with potentially resectable stage II-IV (AJCC 8th) GBC examined at our institution between January 2012 and December 2016. Receiver operating characteristic (ROC) curve analysis was used to determine the predictive value and optimal cut-off point of tumor-associated biomarkers for curative resection. RESULTS Pathological examination of the 309 patients included in this study found that 169 (54.7%) underwent R0 (curative) resection, whereas 121 (39.2%) underwent R1/2 (non-curative) resection, and 19 (6.1%) were unresectable. The mean serum concentrations of CEA, CA19-9 and adjusted CA19-9 were significantly lower in patients who underwent R0 resection than in the other groups. ROC curve analysis showed that adjusted CA19-9 concentration was better able to predict resectability (area under the curve, 0.774; 95% confidence interval, 0.722-0.826; P<0.001) than total bilirubin, CEA, and CA19-9 concentrations. The optimal cut-off for adjusted CA19-9 concentration was 47.63 U/mL, which had a sensitivity of 69.82%, a specificity of 75%, a positive predictive value of 77.12% and a negative predictive value of 67.31%. CONCLUSIONS Adjusted CA19-9 concentration is an easily calculated parameter superior to CA19-9 and CEA concentrations in predicting the resectability of advanced gallbladder cancer.
Conflict of interest statement
None.
Figures

Similar articles
-
Clinical value of preoperative CA19-9 levels in evaluating resectability of gallbladder carcinoma.ANZ J Surg. 2019 Mar;89(3):E76-E80. doi: 10.1111/ans.14893. Epub 2018 Oct 10. ANZ J Surg. 2019. PMID: 30306702
-
Elevation of CA19-9 and CEA is associated with a poor prognosis in patients with resectable gallbladder carcinoma.HPB (Oxford). 2017 Nov;19(11):951-956. doi: 10.1016/j.hpb.2017.06.011. Epub 2017 Jul 24. HPB (Oxford). 2017. PMID: 28750922
-
Can preoperative CA19-9 and CEA levels predict the resectability of patients with pancreatic adenocarcinoma?J Gastroenterol Hepatol. 2009 Dec;24(12):1869-75. doi: 10.1111/j.1440-1746.2009.05935.x. J Gastroenterol Hepatol. 2009. PMID: 19686409
-
Raised CA19-9 and CEA have prognostic relevance in gallbladder carcinoma.BMC Cancer. 2020 Aug 31;20(1):826. doi: 10.1186/s12885-020-07334-x. BMC Cancer. 2020. PMID: 32867709 Free PMC article.
-
[Stomach adenocarcinomas: comparison between CA 19-9 and carcinoembryonic antigen for the diagnosis of recurrences after surgical treatment].Gastroenterol Clin Biol. 1992;16(11):848-52. Gastroenterol Clin Biol. 1992. PMID: 1483553 Review. French.
Cited by
-
The Predictive Roles of Tumour Markers, Hemostasis Assessment, and Inflammation in the Early Detection and Prognosis of Gallbladder Adenocarcinoma and Metaplasia: A Clinical Study.Int J Mol Sci. 2025 Apr 12;26(8):3665. doi: 10.3390/ijms26083665. Int J Mol Sci. 2025. PMID: 40332145 Free PMC article.
-
Radiomics-based machine learning and deep learning to predict serosal involvement in gallbladder cancer.Abdom Radiol (NY). 2024 Jan;49(1):3-10. doi: 10.1007/s00261-023-04029-2. Epub 2023 Oct 3. Abdom Radiol (NY). 2024. PMID: 37787963
-
Noninvasive preoperative differential diagnosis of gallbladder carcinoma and xanthogranulomatous cholecystitis: A retrospective cohort study of 240 patients.Cancer Med. 2022 Jan;11(1):176-182. doi: 10.1002/cam4.4442. Epub 2021 Nov 27. Cancer Med. 2022. PMID: 34837350 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2018;68:394–424. - PubMed
-
- Puhalla H, Wild T, Bareck E, et al. Long-term follow-up of surgically treated gallbladder cancer patients. Eur J Surg Oncol. 2002;28:857–63. - PubMed
-
- Hueman MT, Vollmer CM, Jr, Pawlik TM. Evolving treatment strategies for gallbladder cancer. Ann Surg Oncol. 2009;16:2101–15. - PubMed
-
- Kohya N, Miyazaki K. Hepatectomy of segment 4a and 5 combined with extra-hepatic bile duct resection for T2 and T3 gallbladder carcinoma. J Surg Oncol. 2008;97:498–502. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
