

Non-malarial febrile illness: a systematic review of published aetiological studies and case reports from Africa, 1980-2015
- PMID: 32951596
- PMCID: PMC7504660
- DOI: 10.1186/s12916-020-01744-1
Non-malarial febrile illness: a systematic review of published aetiological studies and case reports from Africa, 1980-2015
Abstract
Background: The availability of reliable point-of-care tests for malaria has heralded a paradigm shift in the management of febrile illnesses away from presumptive antimalarial therapy. In the absence of a definitive diagnosis, health care providers are more likely to prescribe empirical antimicrobials to those who test negative for malaria. To improve management and guide further test development, better understanding is needed of the true causative agents and their geographic variability.
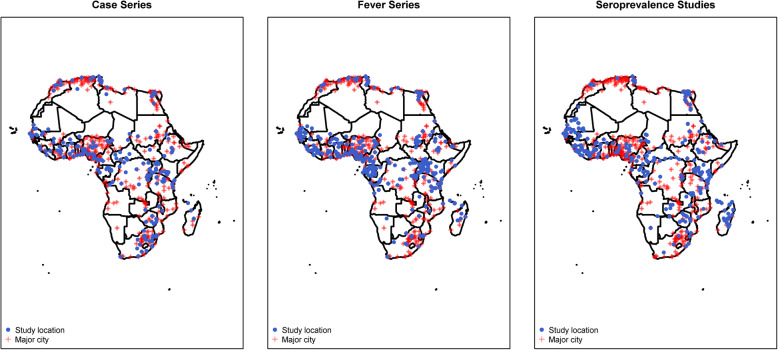
Methods: A systematic review of published literature was undertaken to characterise the spectrum of pathogens causing non-malaria febrile illness in Africa (1980-2015). Literature searches were conducted in English and French languages in six databases: MEDLINE, EMBASE, Global Health (CABI), WHO Global Health Library, PASCAL, and Bulletin de la Société Française de Parasitologie (BDSP). Selection criteria included reporting on an infection or infections with a confirmed diagnosis, defined as pathogens detected in or cultured from samples from normally sterile sites, or serological evidence of current or past infection. A number of published articles (rather than incidence or prevalence) reporting a given pathogen were presented.
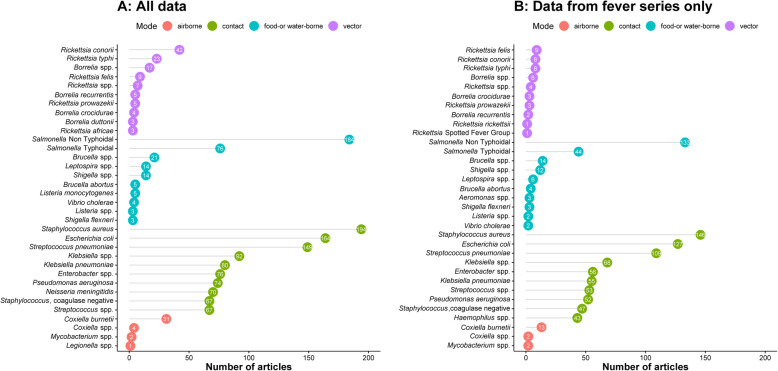
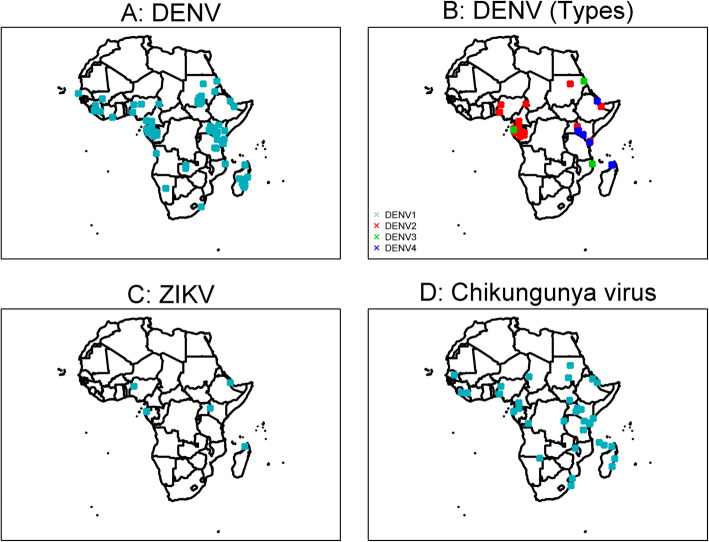
Results: A total of 16,523 records from 48 African countries were screened, of which 1065 (6.4%) met selection criteria. Bacterial infections were reported in 564 (53.0%) records, viral infections in 374 (35.1%), parasitic infections in 47 (4.4%), fungal infections in nine (0.8%), and 71 (6.7%) publications reported more than one pathogen group. Age range of the study population was not specified in 233 (21.9%) publications. Staphylococcus aureus (18.2%), non-typhoidal Salmonella (17.3%), and Escherichia coli (15.4%) were the commonly reported bacterial infections whereas Rift Valley fever virus (7.4%), yellow fever virus (7.0%), and Ebola virus (6.7%) were the most commonly reported viral infections. Dengue virus infection, previously not thought to be widespread in Africa, was reported in 54 (5.1%) of articles.
Conclusions: This review summarises the published reports of non-malaria pathogens that may cause febrile illness in Africa. As the threat of antimicrobial resistance looms, knowledge of the distribution of infectious agents causing fever should facilitate priority setting in the development of new diagnostic tools and improved antimicrobial stewardship.
Trial registration: PROSPERO, CRD42016049281.
Keywords: Aetiology; Africa; Diagnosis; Febrile illness; Fever; Malaria; Microbiology; Non-malarial febrile illness.
Conflict of interest statement
DB and HH were previously employed with FIND, and HH’s salary at LSHTM was previously covered through the ACT Consortium, which was funded through a grant from the Bill and Melinda Gates Foundation to the London School of Hygiene and Tropical Medicine. All other authors declare that they have no competing interests.
Figures




References
-
- World Health Organization . Guidelines for the treatment of malaria. 2010.
-
- WHO. WHO informal consulation on fever management in peripheral health care settings: a global review of evidence and practice. 2013. Available: https://www.who.int/malaria/publications/atoz/9789241506489/en/.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
