

Ex vivo cardiovascular magnetic resonance diffusion weighted imaging in congenital heart disease, an insight into the microstructures of tetralogy of Fallot, biventricular and univentricular systemic right ventricle
- PMID: 32951605
- PMCID: PMC7504600
- DOI: 10.1186/s12968-020-00662-8
Ex vivo cardiovascular magnetic resonance diffusion weighted imaging in congenital heart disease, an insight into the microstructures of tetralogy of Fallot, biventricular and univentricular systemic right ventricle
Abstract
Purpose: Common types of congenital heart disease exhibit a variety of structural and functional variations which may be accompanied by changes in the myocardial microstructure. We aimed to compare myocardial architecture from magnetic resonance diffusion tensor imaging (DTI) in preserved pathology specimens.
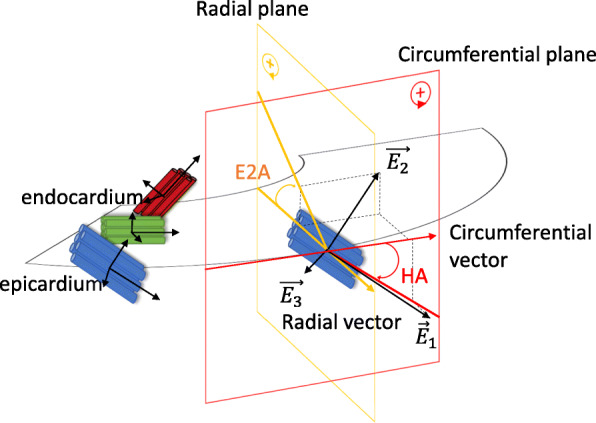
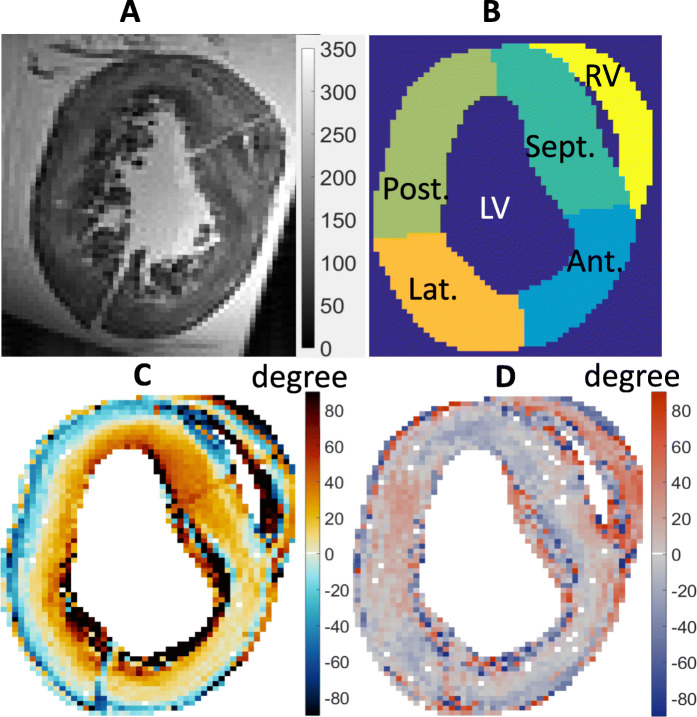
Materials and methods: Pathology specimens (n = 24) formalin-fixed for 40.8 ± 7.9 years comprised tetralogy of Fallot (TOF, n = 10), dextro-transposition of great arteries (D-TGA, n = 8) five with ventricular septal defect (VSD), systemic right ventricle (n = 4), situs inversus totalis (SIT, n = 1) and levo-TGA (L-TGA, n = 1). Specimens were imaged using a custom spin-echo sequence and segmented automatically according to tissue volume fraction. In each specimen T1, T2, fractional anisotropy, mean diffusivity, helix angle (HA) and sheet angle (E2A) were quantified. Pathologies were compared according to their HA gradient, HA asymmetry and E2A mean value in each myocardial segment (anterior, posterior, septal and lateral walls).
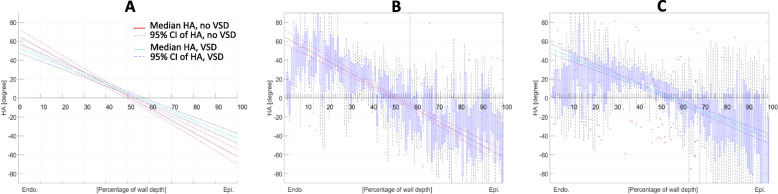
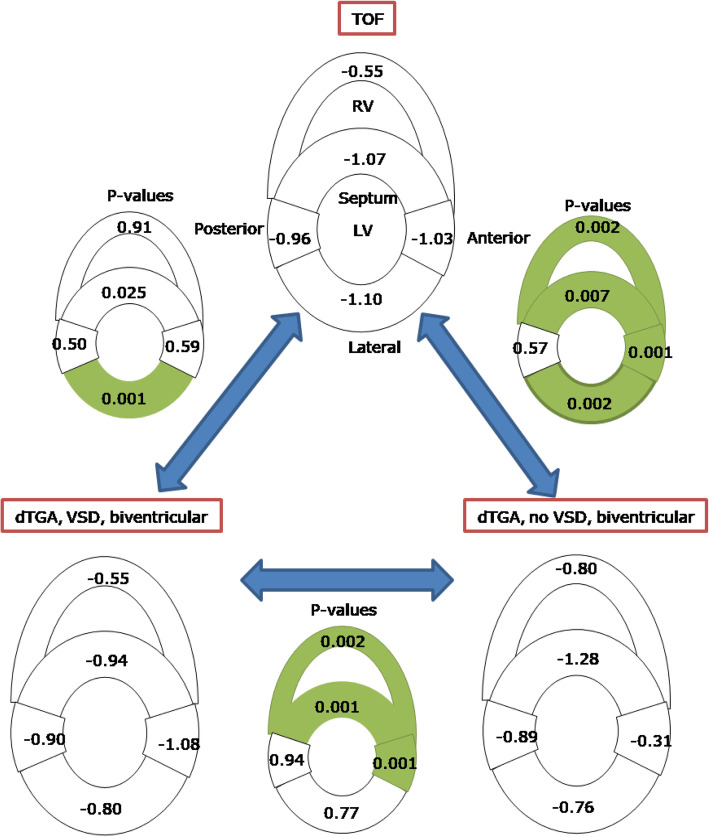
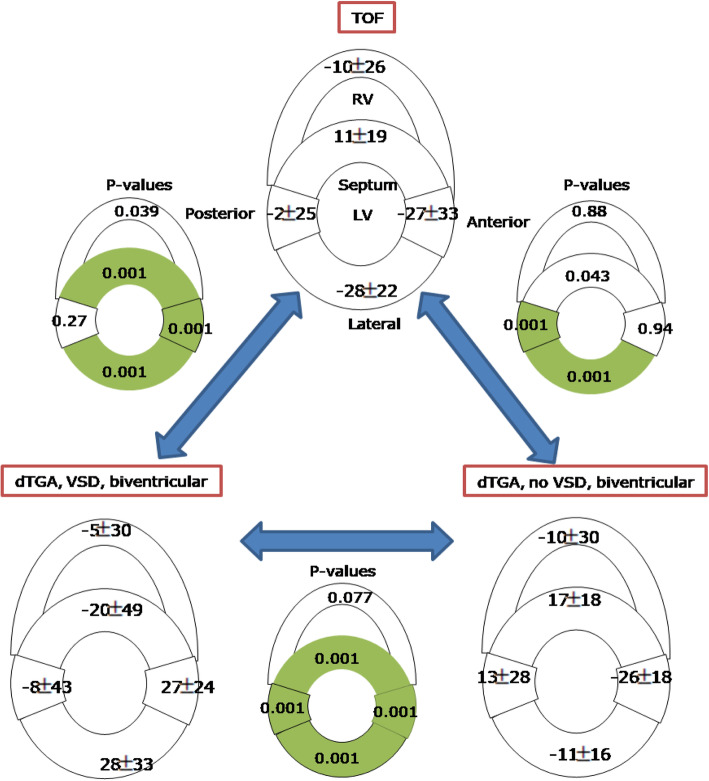
Results: TOF and D-TGA with VSD had decreased helix angle gradient by - 0.34°/% and remained symmetric in the septum in comparison to D-TGA without VSD. Helix angle range was decreased by 45°. It was associated with a decreased HA gradient in the right ventricular (RV) wall, i.e. predominant circumferential myocytes. The sheet angle in the septum of TOF was opposing those of the left ventricular (LV) free wall. Univentricular systemic RV had the lowest HA gradient (- 0.43°/%) and the highest HA asymmetry (75%). HA in SIT was linear, asymmetric, and reversed with a sign change at about 70% of the depth at mid-ventricle. In L-TGA with VSD, HA was asymmetric (90%) and its gradients were decreased in the septum, anterior and lateral wall.
Conclusion: The organization of the myocytes as determined by DTI differs between TOF, D-TGA, L-TGA, systemic RV and SIT specimens. These differences in cardiac structure may further enlighten our understanding of cardiac function in these diverse congenital heart diseases.
Keywords: Congenital heart disease; Dextro; Diffusion tensor imaging; Ex vivo; Levo; Microstructure; Situs inversus; Systemic right ventricle; Tetralogy of Fallot; Transposition of the great arteries; Ventricular septal defect.
Conflict of interest statement
C.T., A.Y, T.G. and B.P declare that they have no competing interests.
Figures

References
-
- Popelová JR, Gebauer R, Černý Š, et al. Operations of adults with congenital heart disease – single center experience with 10 years results. Cor Vasa. 2016;58:e317–e327. doi: 10.1016/J.CRVASA.2015.12.005. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
