

Surgical treatment of high-grade spondylolisthesis: Technique and results
- PMID: 32952331
- PMCID: PMC7486580
- DOI: 10.1016/j.jor.2020.08.015
Surgical treatment of high-grade spondylolisthesis: Technique and results
Abstract
Background: Surgical management of high-grade spondylolisthesis is not only challenging but also controversial, from in situ fusion to complete reduction. We report our results of a safe three-stage spinal procedure in a single surgical session with seven patients diagnosed high-grade spondylolisthesis.
Hypothesis: Posterior fixation combined with interbody fusion is effective on reduction, ossification and clinical outcomes in high-grade spondylolisthesis.
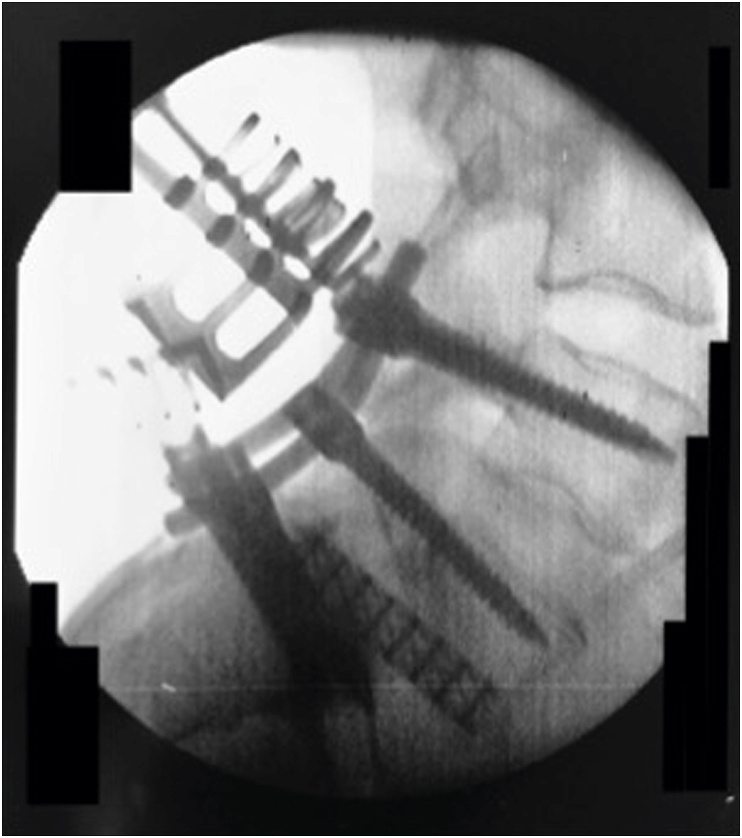
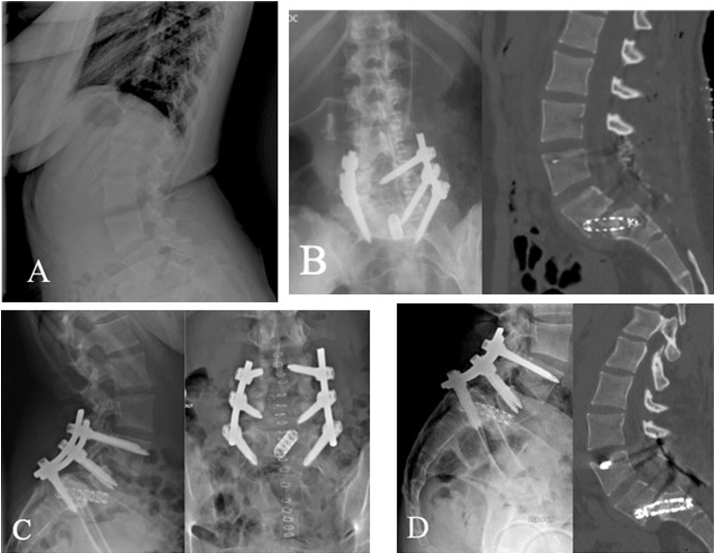
Patients and methods: This study is a retrospective review of patients who underwent surgery between 2016 and 2018. The surgical method involved specific installation for deformity reduction, pedicle screw fixation, correction of lumbosacral kyphosis with a specific distraction maneuver, wide decompression, gradual reduction of the deformity, and sometimes maintenance of the reduction with interbody fusion. Patients were checked out at 2, 6 and 12 months and yearly after the procedure. Clinical, radiological, Visual Analogic Scale (VAS) and Oswestry Disability Index (ODI) outcomes measures were collected.
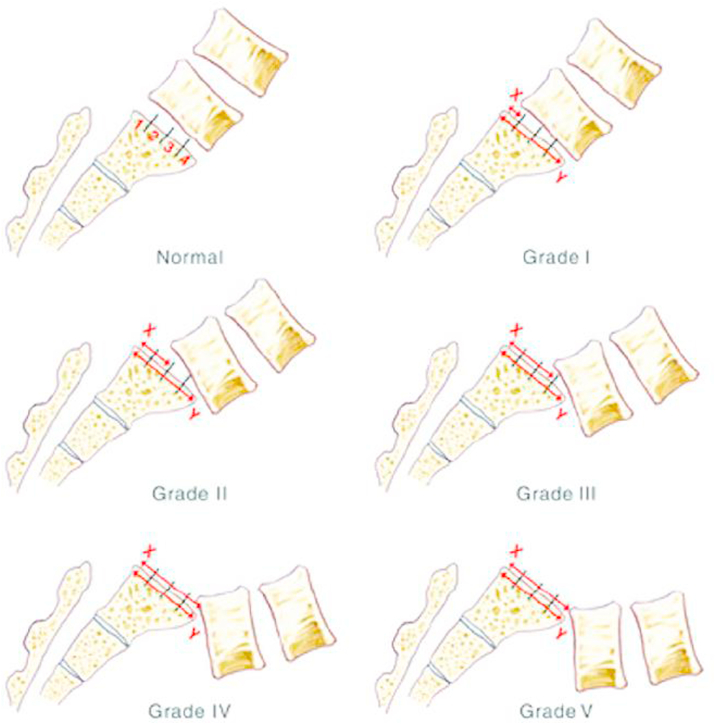
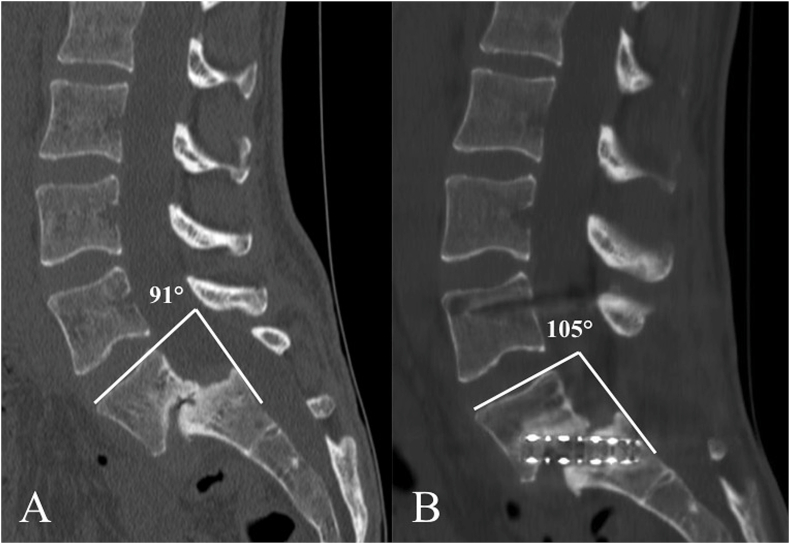
Results: Seven patients with high-grade spondylolisthesis at L5-S1 (2 patients grade II, 4 patients grade IV and 1 patient grade V), with a median age of 37 years [17; 72] were included. Median follow-up was 24 months [12; 25 months]. All patients have a fused joint at 6 months except one. Median lumbosacral angle (LSA) improved from 76°[59; 85] to 94°[76; 104]. Meyerding grade of 2 cases was stable after surgery, 3 cases with loss of two ranks and 2 cases with loss of one rank. The radiological parameters showed statistically significant difference (p = 0.036) postoperatively. There was not deep infection. Medians VAS and ODI showed improved pain and disability scores.
Conclusion: This procedure allows correct reduction rate of high-grade spondylolisthesis with good clinic-radiologic outcomes. Though surgically demanding, it was safe and reproducible.
Level of evidence: IV, retrospective.
Keywords: High-grade spondylolisthesis; Lumbosacral kyphosis; Pedicle screw; Reduction; Sciatalgia; Trans-sacral.
© 2020 Professor P K Surendran Memorial Education Foundation. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
We have not links of interest.
Figures

Similar articles
-
Long-Term Experience With Reduction Technique in High-Grade Spondylolisthesis in the Young.Int J Spine Surg. 2018 Aug 15;12(3):399-407. doi: 10.14444/5047. eCollection 2018 Jun. Int J Spine Surg. 2018. PMID: 30276098 Free PMC article.
-
Transvertebral Transsacral strut grafting for high-grade isthmic spondylolisthesis L5-S1 with fibular allograft.J Spinal Disord Tech. 2008 Jul;21(5):328-33. doi: 10.1097/BSD.0b013e318149e7ea. J Spinal Disord Tech. 2008. PMID: 18600142
-
One-stage posterior spinal shortening by L5 partial spondylectomy for spondyloptosis or L5-S1 high-grade spondylolisthesis management.Eur Spine J. 2016 Feb;25(2):664-70. doi: 10.1007/s00586-015-4174-9. Epub 2015 Aug 14. Eur Spine J. 2016. PMID: 26272371
-
Minimally Invasive Surgery for Managing Grade IV and V Spondylolisthesis.Asian J Neurosurg. 2023 Sep 22;18(3):437-443. doi: 10.1055/s-0043-1771317. eCollection 2023 Sep. Asian J Neurosurg. 2023. PMID: 38152513 Free PMC article. Review.
-
A systematic review of clinical outcomes in surgical treatment of adult isthmic spondylolisthesis.Spine J. 2018 Aug;18(8):1441-1454. doi: 10.1016/j.spinee.2018.04.022. Epub 2018 May 7. Spine J. 2018. PMID: 29746966
Cited by
-
A novel less invasive endoscopic-assisted procedure for complete reduction of low-and high-grade isthmic spondylolisthesis performed by anterior and posterior combined approach.Eur Spine J. 2023 Aug;32(8):2819-2827. doi: 10.1007/s00586-023-07666-9. Epub 2023 Mar 31. Eur Spine J. 2023. PMID: 37000218
-
High-grade dysplastic spondylolisthesis: surgical technique and case series.Musculoskelet Surg. 2023 Sep;107(3):323-331. doi: 10.1007/s12306-022-00763-w. Epub 2022 Oct 1. Musculoskelet Surg. 2023. PMID: 36183053 Free PMC article.
-
Isthmic Spondylolisthesis in Young Gymnasts: A Report of Two Cases.Cureus. 2023 Feb 18;15(2):e35152. doi: 10.7759/cureus.35152. eCollection 2023 Feb. Cureus. 2023. PMID: 36950005 Free PMC article.
-
[Progress in treatment of high-grade spondylolisthesis].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Feb 15;38(2):226-233. doi: 10.7507/1002-1892.202309051. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38385237 Free PMC article. Review. Chinese.
-
Role of Surgeon Demographic Factors in the Management of L4-5 Grade I Spondylolisthesis: A Survey by the AO Spine Knowledge Forum Degenerative.Global Spine J. 2025 Mar 19:21925682251324469. doi: 10.1177/21925682251324469. Online ahead of print. Global Spine J. 2025. PMID: 40105299 Free PMC article.
References
-
- Meyerding H. Spondylolisthesis: surgical treatment and results. Surg Gynecol Obstet. 1932;54:371–377.
-
- Fredrickson B., Baker D., McHolick W. The natural history of spondylolysis and spondylolisthesis. J Bone Jt Surg. 1984;66:699–707. - PubMed
-
- Micheli L.J., Wood R. Back pain in young athletes: significant differences from adults in causes and patterns. Arch Pediatr Adolesc Med. 1995;149:15–18. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
