

Placental Malaria
- PMID: 32953387
- PMCID: PMC7493061
- DOI: 10.1007/s40475-020-00213-2
Placental Malaria
Abstract
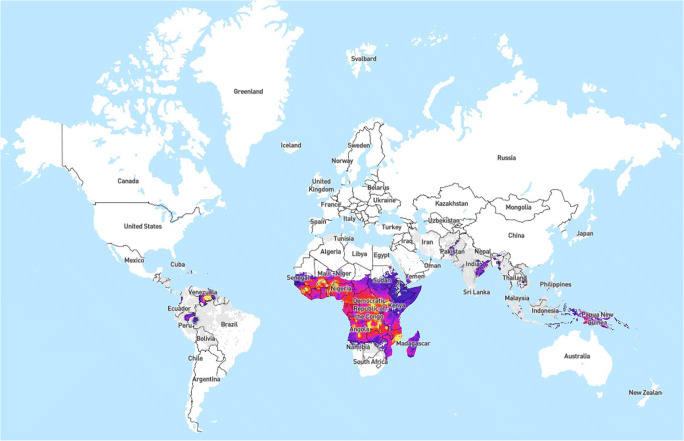
Purpose of review: Placental malaria is the primary mechanism through which malaria in pregnancy causes adverse perinatal outcomes. This review summarizes recent work on the significance, pathogenesis, diagnosis, and prevention of placental malaria.
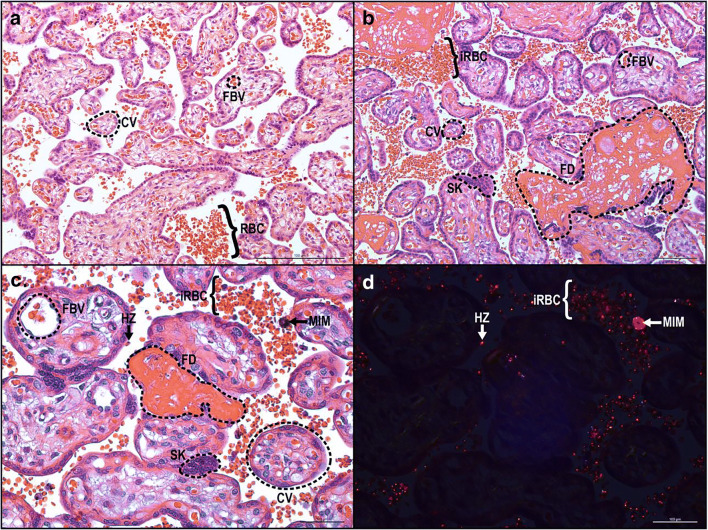
Recent findings: Placental malaria, characterized by the accumulation of Plasmodium-infected red blood cells in the placental intervillous space, leads to adverse perinatal outcomes such as stillbirth, low birth weight, preterm birth, and small-for-gestational-age neonates. Placental inflammatory responses may be primary drivers of these complications. Associated factors contributing to adverse outcomes include maternal gravidity, timing of perinatal infection, and parasite burden.
Summary: Placental malaria is an important cause of adverse birth outcomes in endemic regions. The main strategy to combat this is intermittent preventative treatment in pregnancy; however, increasing drug resistance threatens the efficacy of this approach. There are studies dissecting the inflammatory response to placental malaria, alternative preventative treatments, and in developing a vaccine for placental malaria.
Keywords: Malaria in pregnancy; Obstetrical outcomes of placental malaria; Pathogenesis of placental malaria; Placental malaria; Plasmodium infection; Prevention of placental malaria.
© Springer Nature Switzerland AG 2020.
Conflict of interest statement
Conflict of InterestThe authors declare that they have no conflict of interest.
Figures
References
-
- WHO. World Malaria Report 2017. World Health Organization. 2017. 10.1071/EC12504.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials