

Chemical pleurodesis and somatostatin in treating spontaneous chylothorax in pediatric patients: a retrospective analysis and review of the literature
- PMID: 32953553
- PMCID: PMC7475317
- DOI: 10.21037/tp-20-199
Chemical pleurodesis and somatostatin in treating spontaneous chylothorax in pediatric patients: a retrospective analysis and review of the literature
Abstract
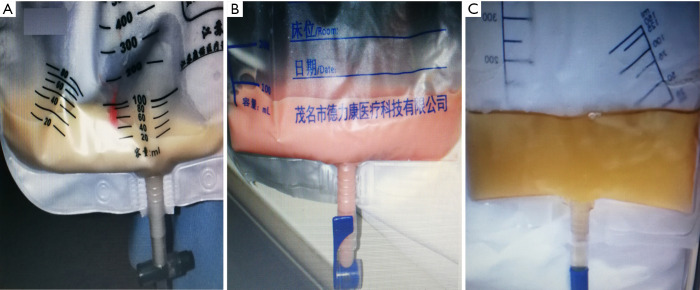
Background: Chylothorax is a rare disease, defined as an abnormal accumulation of chylous lymphatic effusion in thoracic cavity, with a high mortality rate in pediatric patients. At present, there are few studies on the treatment of pediatric chylothorax, and conservative treatments like somatostatin (SST) and pleurodesis are performed empirically. SST has been used for treating pediatric chylothorax over 20 years, and povidone-iodine chemical pleurodesis (PICP) is adopted in recent years with a high cure rate, but both the effect are still uncertain. The safety and efficacy of SST and PICP in treating pediatric chylothorax was compared in this study.
Methods: From January 2009 to May 2020, 27 pediatric chylothorax patients who accepted life support, SST and PICP treatment were retrospectively reviewed in this study. Their medical history, clinical manifestations, pleural effusion examinations, treatment methods, effects, and complications were screened. PICP and SST was performed in 19 and 8 children, respectively. Each patient was followed up after discharge from the hospital.
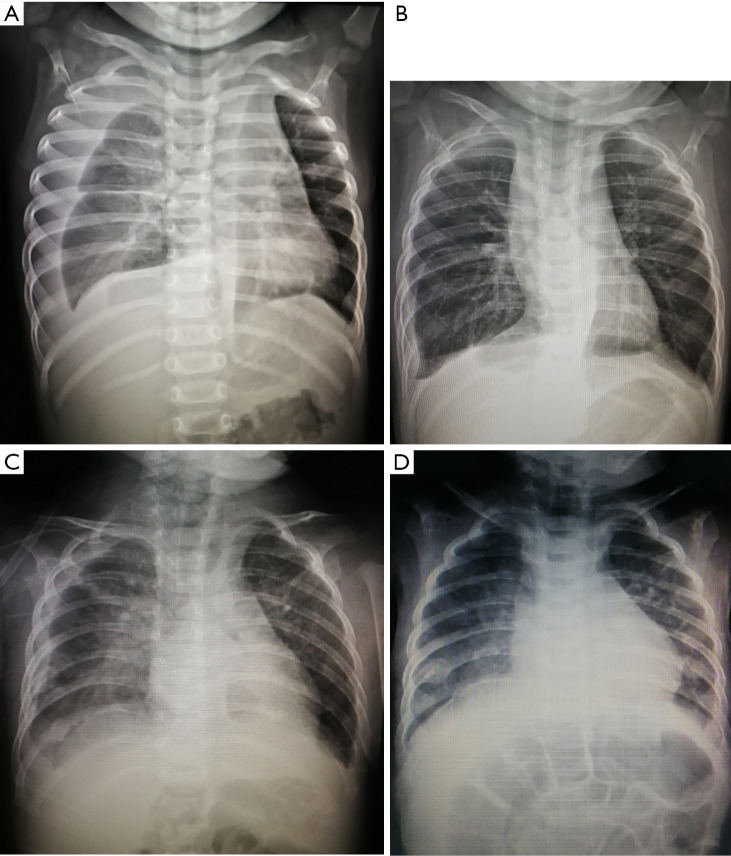
Results: After admission, chest X-ray and ultrasound diagnosed pleural effusion in 27 patients (18 males and 9 females), including 13 and 6 cases on the left and right side, and 8 cases on both sides. In the pleural effusion, the mean leukocyte count was (9,826±9,482)×106/L, the mean lymphocyte ratio was (84.82±6.58)%, the mean triglyceride content was 7.11±6.63 mmol/L. In PICP and SST group, the mean length of stay was 38.42±19.42 and 35.13±12.72 d (P=0.664), the mean time of thoracic drainage was 24.58±16.34 and 19.63±8.88 d (P=0.440), the mean time of parenteral nutrition was 27.16±18.29 and 25.25±13.52 d (P=0.793), respectively. PICP was performed for 3.16±2.27 times, and SST was used for 14.75±9.08 d with the dosage of 0.5 to 10 µg/kg/hour. After the treatment, all patients in PICP group had mild chest pain and low-grade fever, and 12 cases were observed with transient decrease of oxygen saturation. Eight patients in SST group had nausea and vomit, and 1 child had diarrhea simultaneously. Both were cured by symptomatic treatment, thoracic drainage and discontinuing using SST. Three children were diagnosed with refractory chylothorax and cured by PICP after SST. Pleural effusion in 27 patients was finally absorbed. All of them achieved a clinical cure successfully, and there was no recurrence during discharge follow-up.
Conclusions: PICP has a high success rate and few adverse reactions in treating spontaneous chylothorax in pediatric patients, expected to be a new treatment option for pediatric chylothorax after SST.
Keywords: Chylothorax; pleural effusion; pleurodesis; povidone-iodine (PI); somatostatin (SST).
2020 Translational Pediatrics. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tp-20-199). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous