

Uniportal video-assisted thoracoscopic thymectomy: the glove-port with carbon dioxide insufflation
- PMID: 32953596
- PMCID: PMC7475351
- DOI: 10.21037/gs-19-521
Uniportal video-assisted thoracoscopic thymectomy: the glove-port with carbon dioxide insufflation
Abstract
Background: Since 2004, uniportal video-assisted thoracic surgery (VATS) approach was progressively widespread and also applied in the treatment of thymoma, with promising results. We report the first series of patients who undergone uniportal VATS thymectomy using a homemade glove-port with carbon dioxide (CO2) insufflation. The aim of this article is to analyze the safety and feasibility to perform an extended thymectomy (ET).
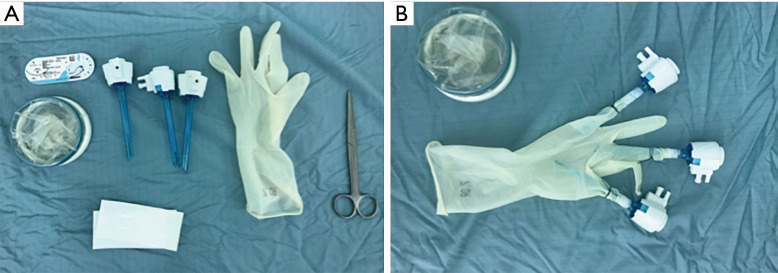
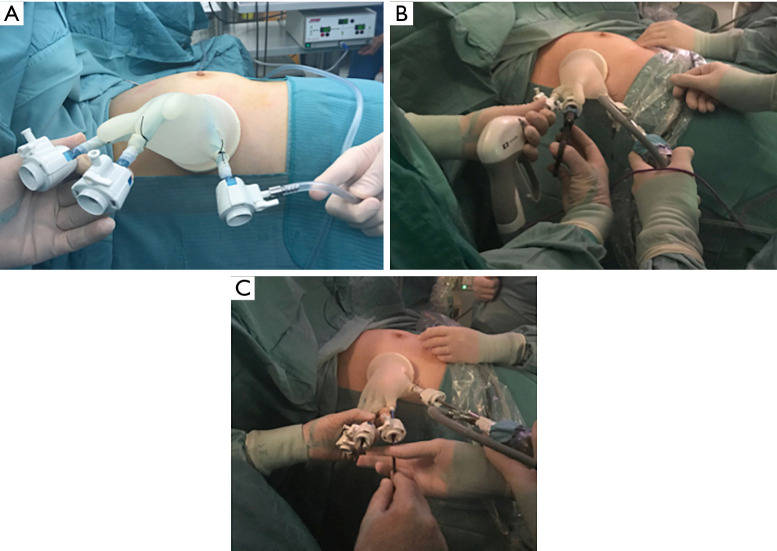
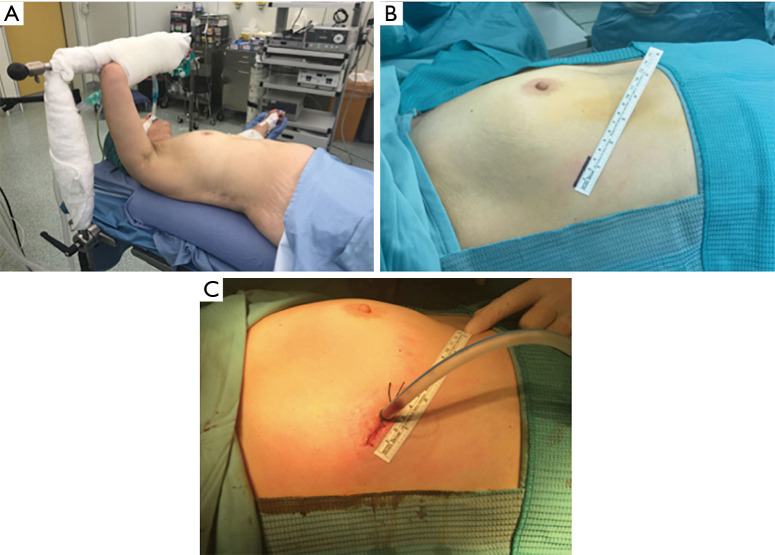
Methods: A prospective, single-centre, short-term observational study including patients with mediastinal tumours undergoing scheduled uniportal VATS resection using a glove-port with CO2. Operations were performed through a single incision of 3.5 cm at the fifth intercostal space, right or left anterior axillary line. A 5 mm-30° camera and working instruments were employed through a glove-port with CO2.
Results: Thirty-eight patients (20 men; mean age 61.6 years) underwent ET between September 2016 and October 2019. Thirteen patients had a history of Myasthenia Gravis (MG) with thymoma and 8 had incidental findings of thymoma. Additionally, 8 mediastinal cysts and 9 thymic hyperplasia were included. Mean diameter of the tumor was 5.1 cm (range, 1.6-14 cm) and mean operation time was 143 minutes. Mean postoperative drainage duration and hospital stay were 2.3 and 4.3 days, respectively. Mean blood loss was 41 mL. There was no occurrence of surgical morbidity or mortality. During the follow-up period (1-36 months), no recurrence was noted.
Conclusions: Our results suggest that uniportal VATS thymectomy through glove-port and CO2 is safe and feasible procedure, even with large thymomas. Furthermore, the glove-port system represents a valid, cheap and widely available alternative to the commercial devices usually adopted in thoracic surgery.
Keywords: Glove-port; myasthenia gravis (MG); thymectomy; uniportal video-assisted thoracoscopic thymectomy; video-assisted thoracic surgery (VATS).
2020 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/gs-19-521). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources