

Etiologies, Clinical Features, and Outcome of Oxalate Nephropathy
- PMID: 32954074
- PMCID: PMC7486173
- DOI: 10.1016/j.ekir.2020.06.021
Etiologies, Clinical Features, and Outcome of Oxalate Nephropathy
Abstract
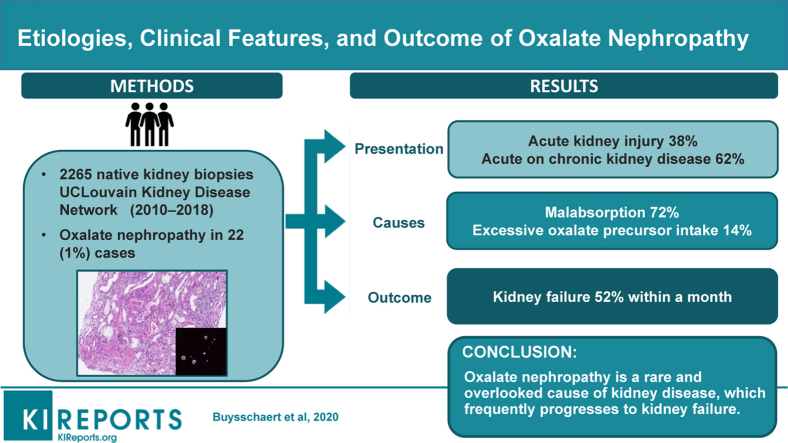
Background: Oxalate nephropathy is a potentially underestimated cause of kidney failure characterized by massive deposition of calcium oxalate crystals in the renal parenchyma. The prevalence and modes of presentation of this entity are ill-defined.
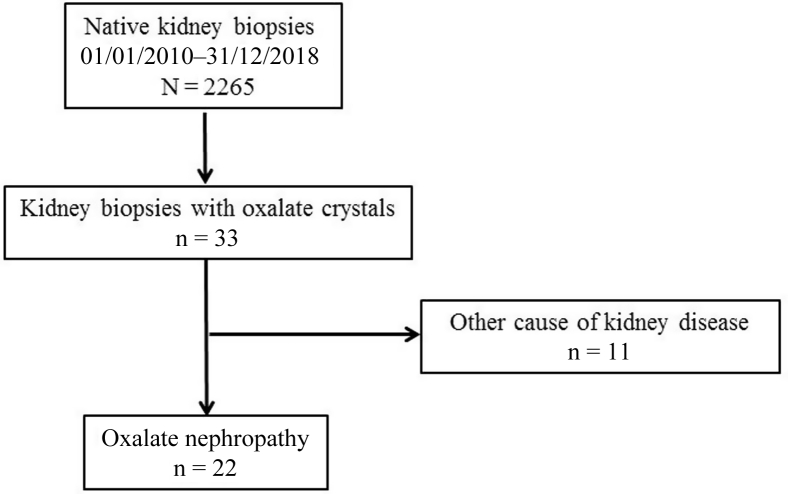
Methods: Here we report on the largest consecutive series of cases of adult oxalate nephropathy diagnosed on native kidney biopsies from January 2010 to December 2018 in the UCLouvain Kidney Disease Network.
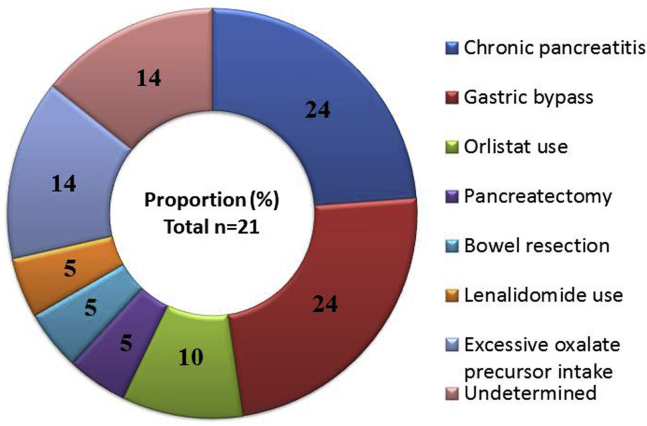
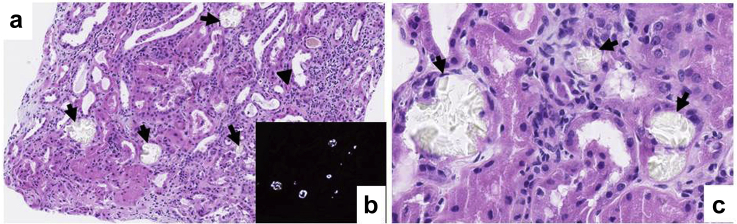
Results: We screened 2265 native kidney biopsies and identified 22 cases (1%) of oxalate nephropathy. Patients had a mean age at diagnosis of 61 years (±20) and presented either with acute on chronic kidney disease (CKD) (62%) or with acute kidney injury (AKI) (38%). Mean serum creatinine at biopsy was 8.0 ± 4.5 mg/dl. Kidney biopsies showed abundant calcium oxalate crystal deposits, associated with acute interstitial nephritis and tubular necrosis, and variable degrees of interstitial fibrosis and tubular atrophy. Chronic pancreatitis and gastric bypass were the most common causes of oxalate nephropathy (48%). During a mean follow-up of 29 months, half of the patients (52%) progressed to kidney failure, all within the month following diagnosis. Higher serum creatinine level at presentation and interstitial fibrosis and tubular atrophy score were associated with progression to kidney failure.
Conclusion: Oxalate nephropathy is the cause of kidney disease in 1% of consecutive native kidney biopsies and typically presents as acute on CKD or AKI. The prognosis of the disease is poor, with a high rate of kidney failure within the first month after the diagnosis.
Keywords: chronic pancreatitis; fat malabsorption; gastric bypass; hyperoxaluria; steatorrhea.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Cochat P., Rumsby G. Primary hyperoxaluria. N Engl J Med. 2013;369:649–658. - PubMed
LinkOut - more resources
Full Text Sources
