

Dependence, withdrawal and rebound of CNS drugs: an update and regulatory considerations for new drugs development
- PMID: 32954266
- PMCID: PMC7425303
- DOI: 10.1093/braincomms/fcz025
Dependence, withdrawal and rebound of CNS drugs: an update and regulatory considerations for new drugs development
Abstract
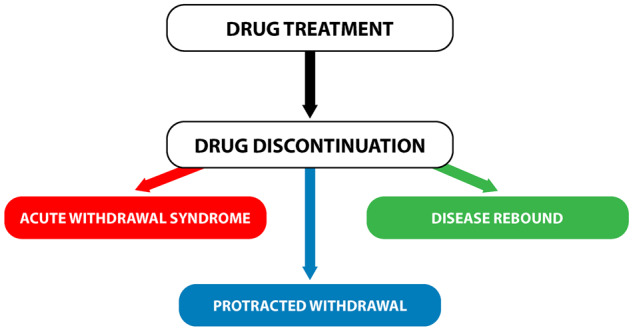
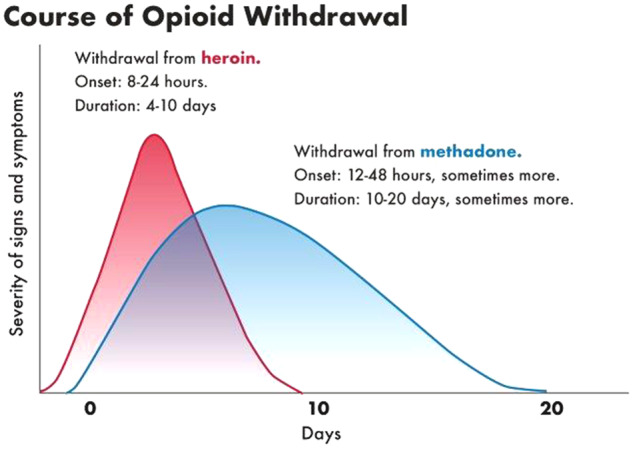
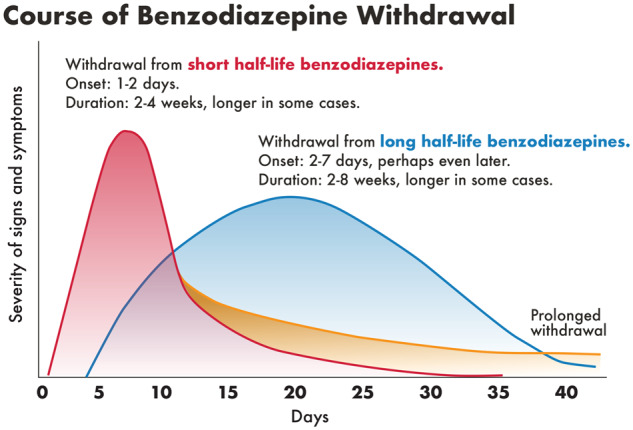
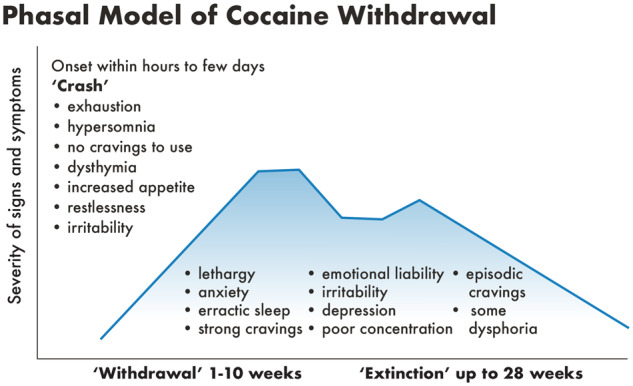
The purpose of this article is to describe dependence and withdrawal phenomena related to CNS drugs discontinuation and to clarify issues related to the evaluation of clinical drug withdrawal and rebound as they relate to safety in new drug development. The article presents current understanding and definitions of drug dependence and withdrawal which are also relevant and important features of addiction, though not the same. Addiction, called substance use disorder in DSM-5, affects an individual's brain and behaviour, represents uncontrollable drug abuse and inability to stop taking a drug regardless of the harm it causes. Characteristic withdrawal syndromes following abrupt discontinuation of CNS-active drugs from numerous drug classes are described. These include drugs both scheduled and non-scheduled in the Controlled Substances Act, which categorizes drugs in five schedules based on their relative abuse potentials and dependence liabilities and for regulatory purposes. Schedules 1 and 2 contain drugs identified as those with the highest abuse potential and strictest regulations. Less recognized aspects of drug withdrawal, such as rebound and protracted withdrawal syndromes for several drug classes are also addressed. Part I presents relevant definitions and describes clinical withdrawal and dependence phenomena. Part II reviews known withdrawal syndromes for the different drug classes, Part III describes rebound and Part IV describes protracted withdrawal syndromes. To our knowledge, this is the first compilation of withdrawal syndromes for CNS drugs. Part V provides details of evaluation of dependence and withdrawal in the clinical trials for CNS drugs, which includes general design recommendations, and several tools, such as withdrawal questionnaires and multiple scales that are helpful in the systematic evaluation of withdrawal. The limitations of different aspects of this method of dependence and withdrawal evaluation are also discussed.
Keywords: dependence; human dependence evaluation; rebound; withdrawal syndromes.
© The Author(s) (2019). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Agrawal A, Pergadia ML, Lynskey MT.. Is there evidence for symptoms of cannabis withdrawal in the national epidemiologic survey of alcohol and related conditions? Am J Addict 2008; 17: 199–208. - PubMed
-
- Amore M, Zazzeri N.. Neuroleptic malignant syndrome after neuroleptic discontinuation. Prog Neuropsychopharmacol Biol Psychiatry 1995; 19: 1323–34. - PubMed
-
- Anand KJ, Ingraham J.. Pediatric. Tolerance, dependence, and strategies for compassionate withdrawal of analgesics and anxiolytics in the pediatric ICU. Crit Care Nurse 1996; 16: 87–93. - PubMed
-
- APA. Diagnostic and statistical manual of mental disorders, 5th Edition: DSM-5. 5th edn.Arlington, VA: American Psychiatric Publishing; 2013.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources