

Quantitative Corticospinal Tract Assessment in Acute Intracerebral Hemorrhage
- PMID: 32954472
- PMCID: PMC8213667
- DOI: 10.1007/s12975-020-00850-9
Quantitative Corticospinal Tract Assessment in Acute Intracerebral Hemorrhage
Abstract
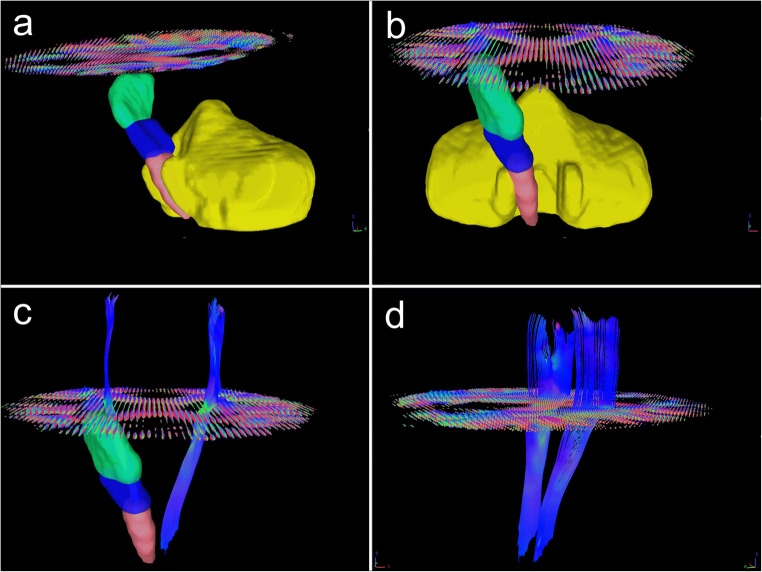
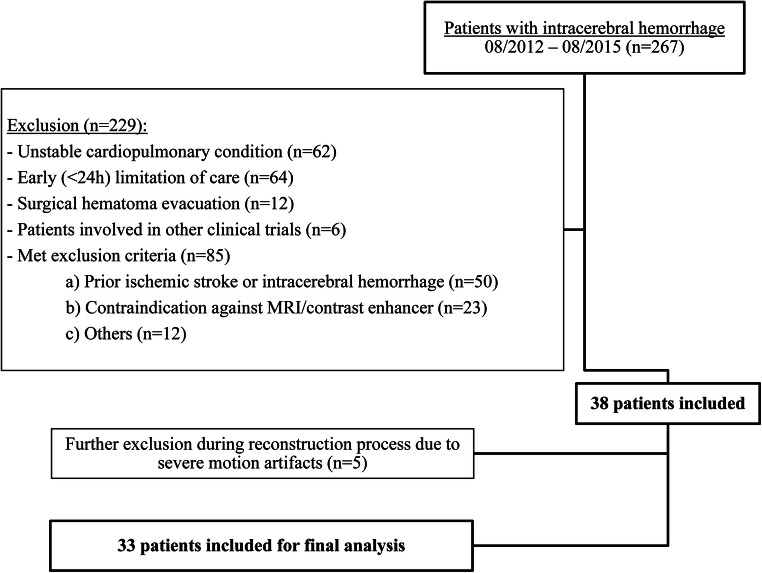
Intracerebral hemorrhage (ICH) prognostication during the acute phase is often subjective among physicians and often affects treatment decisions. The present study explores objective imaging parameters using quantitative corticospinal tract (CST) fiber reconstruction during the acute phase of ICH and correlates these parameters with functional outcome and patient recovery. We prospectively enrolled nonsurgical spontaneous supratentorial ICH patients and obtained an MRI scan on day 5 ± 1. Q-space diffeomorphic reconstruction was performed using DSI Studio, and quantitative anisotropy (QA) was calculated. The CST was reconstructed based on QA. The dichotomized modified Rankin Scale score on day 90 (favorable outcome = 0-2) and Barthel Index (favorable recovery = 100 on day 90 or improvement between discharge and day 90 > 60%) were assessed. Thirty-three patients, median age 72 years (interquartile range (IQR) 64-83), 21 female (64%), 21 (64%) with lobar hemorrhage, median ICH volume on admission 15.0 (IQR 7.0-27.4) mL, were included. Sixteen patients (48%) had a favorable outcome and 24 (73%) had a favorable recovery. The mean number of ipsilesional reconstructed CST fiber pathways was higher in patients with favorable outcomes (153 (standard deviation (SD) 103) vs. 60 (SD 39), p = 0.003) and predicted outcome after adjustment (Exp(B) = 1.016 (95% CI = 1.002-1.030)). QA in the ipsilesional posterior limb of the internal capsule showed a trend towards an association with favorable outcome (Exp(B) = 1.194 (95% CI = 0.991-1.439 (adjusted))). The total (ipsilesional + contralesional) number of reconstructed fiber pathways was associated with favorable recovery (Exp(B) = 1.025 (95% CI = 1.003-1.047 (adjusted))). Quantitative tractography parameters assessed in the acute phase of ICH may represent a promising predictor of long-term outcome and recovery. This might facilitate prognostic evaluation and organization of rehabilitation.
Keywords: All rehabilitation; DWI; Intracerebral hemorrhage; MRI; Outcome research.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Venkatasubramanian C, Kleinman JT, Fischbein NJ, Olivot JM, Gean AD, Eyngorn I, Snider RW, Mlynash M, Wijman CAC. Natural history and prognostic value of corticospinal tract Wallerian degeneration in intracerebral hemorrhage. J Am Heart Assoc. 2013;2(4):e000090. doi: 10.1161/JAHA.113.000090. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
