

Effects of Home-Based Cardiac Rehabilitation on Time to Enrollment and Functional Status in Patients With Ischemic Heart Disease
- PMID: 32954885
- PMCID: PMC7792373
- DOI: 10.1161/JAHA.120.016456
Effects of Home-Based Cardiac Rehabilitation on Time to Enrollment and Functional Status in Patients With Ischemic Heart Disease
Abstract
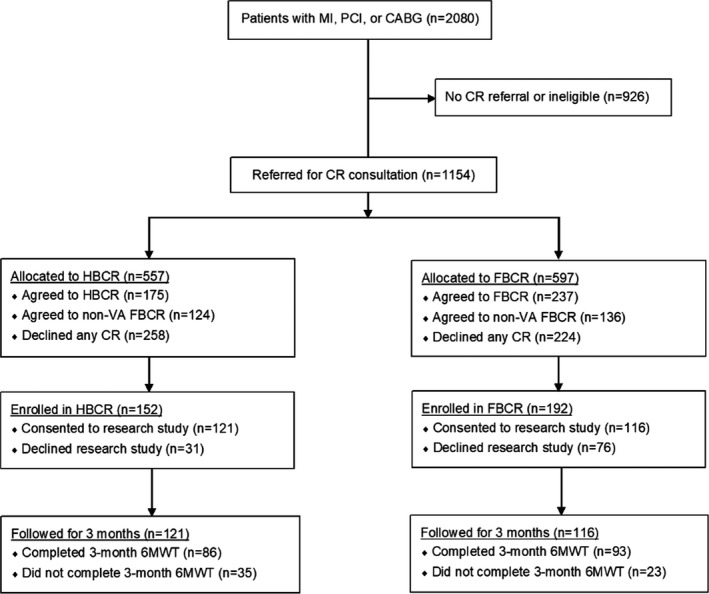
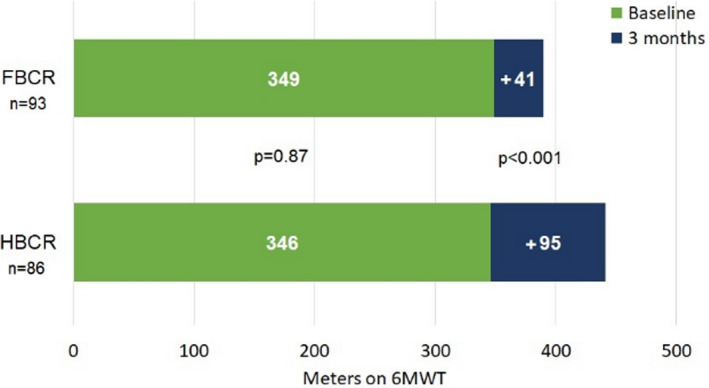
Background Cardiac rehabilitation is an established performance measure for adults with ischemic heart disease, but patient participation is remarkably low. Home-based cardiac rehabilitation (HBCR) may be more practical and feasible, but evidence regarding its efficacy is limited. We sought to compare the effects of HBCR versus facility-based cardiac rehabilitation (FBCR) on functional status in patients with ischemic heart disease. Methods and Results This was a pragmatic trial of 237 selected patients with a recent ischemic heart disease event, who enrolled in HBCR or FBCR between August 2015 and September 2017. The primary outcome was 3-month change in distance completed on a 6-minute walk test. Secondary outcomes included rehospitalization as well as patient-reported physical activity, quality of life, and self-efficacy. Characteristics of the 116 patients enrolled in FBCR and 121 enrolled in HBCR were similar, except the mean time from index event to enrollment was shorter for HBCR (25 versus 77 days; P<0.001). As compared with patients undergoing FBCR, those in HBCR achieved greater 3-month gains in 6-minute walk test distance (+95 versus +41 m; P<0.001). After adjusting for demographics, comorbid conditions, and indication, the mean change in 6-minute walk test distance remained significantly greater for patients enrolled in HBCR (+101 versus +40 m; P<0.001). HBCR participants reported greater improvements in quality of life and physical activity but less improvement in exercise self-efficacy. There were no deaths or cardiovascular hospitalizations. Conclusions Patients enrolled in HBCR achieved greater 3-month functional gains than those enrolled in FBCR. Our data suggest that HBCR may safely derive equivalent benefits in exercise capacity and overall program efficacy in selected patients. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02105246.
Keywords: cardiac rehabilitation; exercise; outcomes; telemedicine.
Conflict of interest statement
None.
Figures
References
-
- Smith SC Jr, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, Gibbons RJ, Grundy SM, Hiratzka LF, Jones DW, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation. 2011;2458–2473. - PubMed
-
- Thomas RJ, Balady G, Banka G, Beckie TM, Chiu J, Gokak S, Ho PM, Keteyian SJ, King M, Lui K, et al. 2018 ACC/AHA clinical performance and quality measures for cardiac rehabilitation: a report of the American College of Cardiology/American Heart Association Task Force on performance measures. Circ Cardiovasc Qual Outcomes. 2018;9:e000037 DOI: 10.1161/HCQ.0000000000000037. - DOI - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE Jr, Ganiats TG, Holmes DR Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, et al. 2014 AHA/ACC guideline for the management of patients with non‐ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;e344–e426. - PubMed
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, et al. 2013 ACCF/AHA guideline for the management of ST‐elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;e362–e425. - PubMed
-
- Anderson L, Oldridge N, Thompson DR, Zwisler AD, Rees K, Martin N, Taylor RS. Exercise‐based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta‐analysis. J Am Coll Cardiol. 2016;1–12. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
