

Management of Abemaciclib-Associated Adverse Events in Patients with Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: Safety Analysis of MONARCH 2 and MONARCH 3
- PMID: 32955138
- PMCID: PMC7794176
- DOI: 10.1002/onco.13531
Management of Abemaciclib-Associated Adverse Events in Patients with Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: Safety Analysis of MONARCH 2 and MONARCH 3
Erratum in
-
Management of Abemaciclib-Associated Adverse Events in Patients with Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: Safety Analysis of MONARCH 2 and MONARCH 3.Oncologist. 2021 Mar;26(3):e522. doi: 10.1002/onco.13691. Oncologist. 2021. PMID: 33660385 Free PMC article. No abstract available.
Abstract
Background: Abemaciclib demonstrated efficacy in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer. Here we provide a comprehensive summary of the most common adverse events (AEs), their management, and whether AEs or dose reductions influenced progression-free survival (PFS), in the MONARCH 2 and 3 trials.
Materials and methods: Incidence of the most clinically relevant AEs, management, and outcomes were summarized. Time-dependent covariate analyses examined the impact of dose reductions on PFS. PFS was estimated for patients with and without early onset of diarrhea or neutropenia.
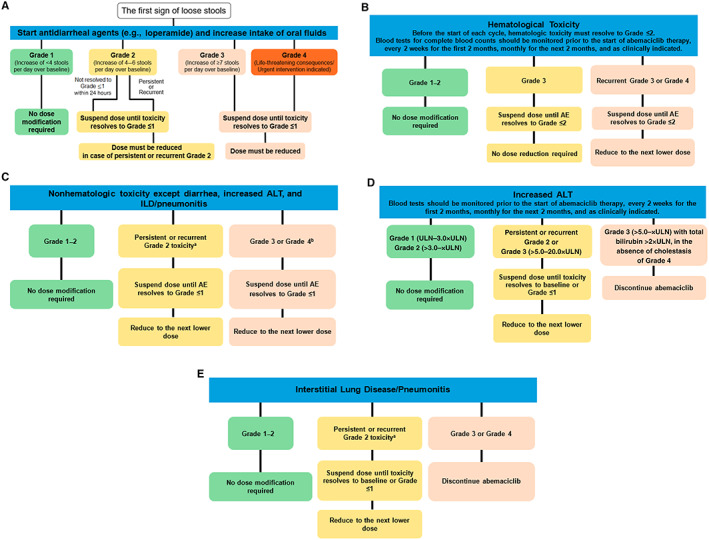
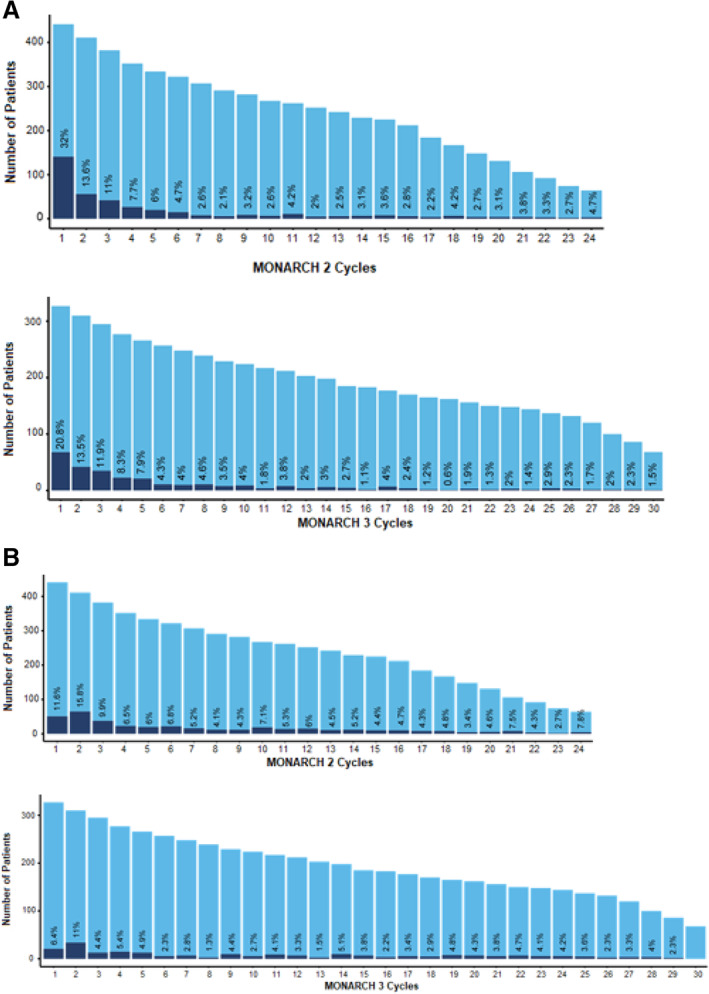
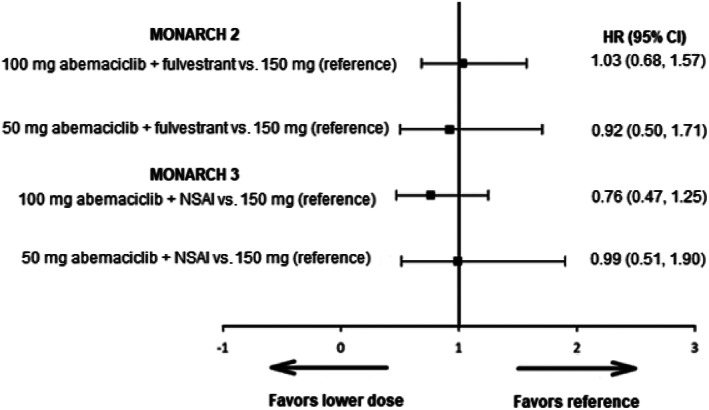
Results: The most frequently reported AE was diarrhea, with clinically significant diarrhea (grade ≥2) reported for 42.8% of patients taking abemaciclib. Median time to onset was 1 week, and duration ranged from 6 to 12 days, depending on grade and study. Diarrhea was adequately managed by antidiarrheal medication (72.8%), dose omissions (17.3%), and reductions (16.7%). The highest rates of grade ≥2 diarrhea were observed in the first cycles and decreased in subsequent cycles. Neutropenia (grade ≥3) occurred in 25.4% of abemaciclib-treated patients. Neutropenia resolved with dose omissions (16.8%) and/or dose reductions (11.2%). Incidence of febrile neutropenia (0.7%) or other relevant grade ≥3 hematological events (<9%) was low. Venous thromboembolic events (5.3%) were primarily treated with anticoagulants. Interstitial lung disease/pneumonitis (3.4%) was treated with corticosteroids and/or antibiotics. PFS benefit of abemaciclib was not impacted by dose reductions or early onset of toxicities.
Conclusion: Abemaciclib was generally well tolerated. The most common AEs were effectively managed by supportive medications, and/or dose adjustments, with no detriment to PFS.
Implications for practice: Treatment with abemaciclib plus fulvestrant or nonsteroidal aromatase inhibitors is generally well tolerated in patients with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer. In MONARCH 2 and MONARCH 3, any-grade diarrhea and grade ≥3 neutropenia were effectively managed with supportive medication and/or dose adjustment. Venous thromboembolic events were treated with anticoagulants and did not often require treatment discontinuation. Interstitial lung disease/pneumonitis was infrequent and treated with corticosteroids and/or antibiotics. Clinicians should be aware of and implement management strategies, including dose adjustments according to local labels, for commonly occurring and serious adverse events to ensure continued treatment and optimize clinical benefit/risk ratio.
Keywords: Abemaciclib; Advanced breast cancer; Diarrhea; Neutropenia; Safety.
© 2020 The Authors. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Conflict of interest statement
Figures
Comment in
-
Regarding the Article by Rugo et al.Oncologist. 2021 Jul;26(7):e1285. doi: 10.1002/onco.13781. Epub 2021 Apr 28. Oncologist. 2021. PMID: 33818868 Free PMC article.
-
In Reply.Oncologist. 2021 Jul;26(7):e1286-e1287. doi: 10.1002/onco.13782. Epub 2021 Apr 19. Oncologist. 2021. PMID: 33826783 Free PMC article.
References
-
- Lumachi F, Luisetto G, Basso SM et al. Endocrine therapy of breast cancer. Curr Med Chem 2011;18:513–522. - PubMed
-
- Sledge GW Jr, Toi M, Neven P et al. MONARCH 2: Abemaciclib in combination with fulvestrant in women with HR+/HER2‐ advanced breast cancer who had progressed while receiving endocrine therapy. J Clin Oncol 2017;35:2875–2884. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
