

Fecal Microbiota Transplantation for Ulcerative Colitis: The Optimum Timing and Gut Microbiota as Predictors for Long-Term Clinical Outcomes
- PMID: 32955197
- PMCID: PMC7431231
- DOI: 10.14309/ctg.0000000000000224
Fecal Microbiota Transplantation for Ulcerative Colitis: The Optimum Timing and Gut Microbiota as Predictors for Long-Term Clinical Outcomes
Abstract
Introduction: The previous researches aimed to evaluate the efficacy and safety of fecal microbiota transplantation (FMT) for ulcerative colitis (UC) in a short-term observation. The present study aimed to explore the optimum timing of FMT for maintaining the long-term clinical benefits and to target the gut microbiota that may help to predict the long-term success or failure of FMT in UC.
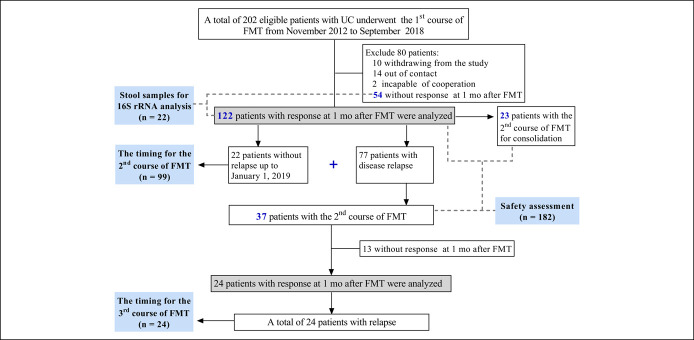
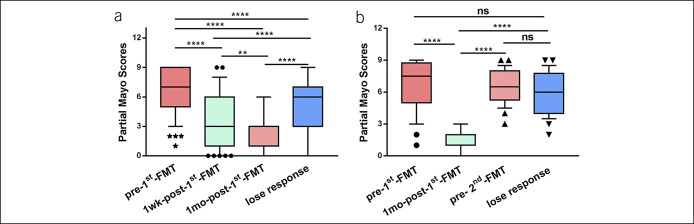
Methods: Two hundred two patients with UC were recruited from November 2012 to September 2018. The primary endpoint of this study was the maintaining time of the first and second courses of FMT. Relapse was defined as partial Mayo score ≥2 after achieving clinical remission and an increase of partial Mayo score ≥1 after achieving clinical response. The stool samples were analyzed by 16S rRNA gene sequencing.
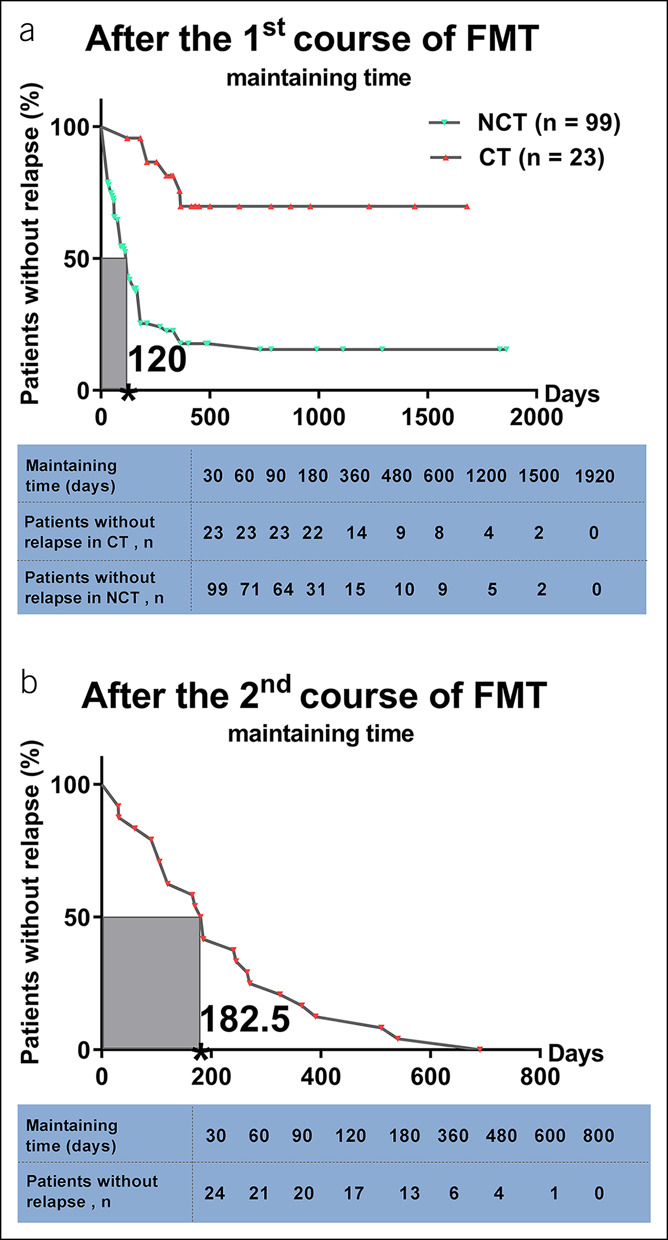
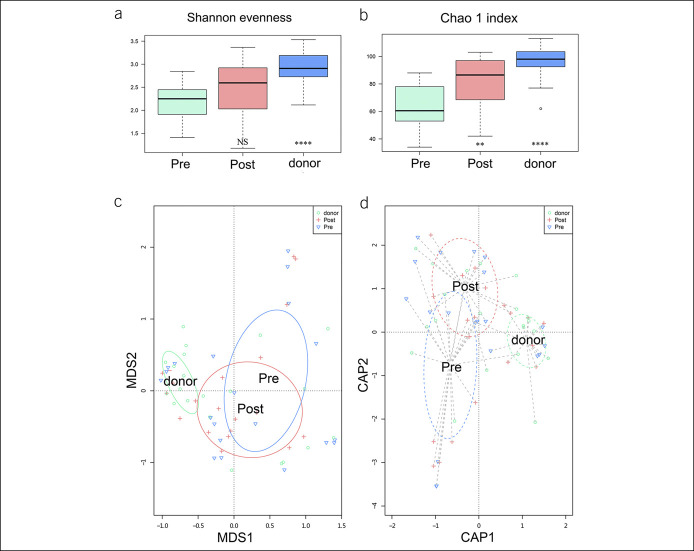
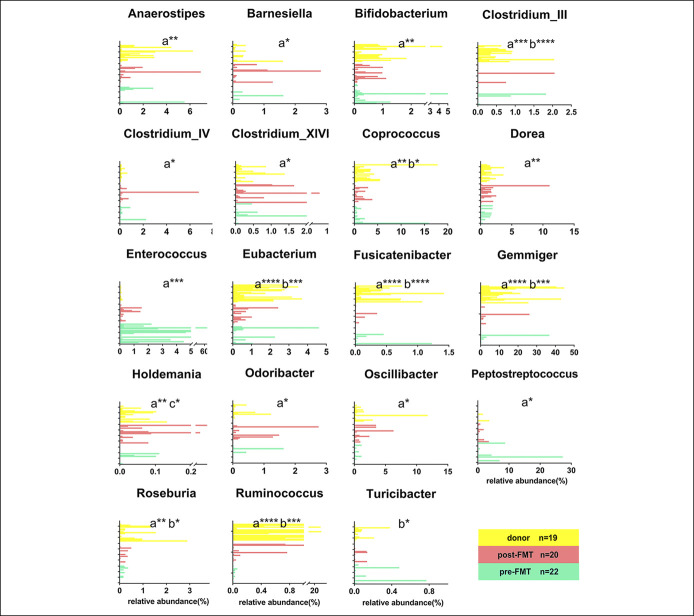
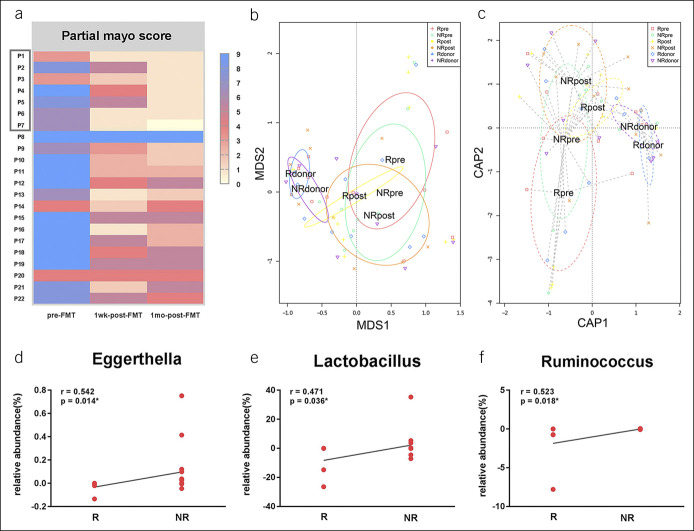
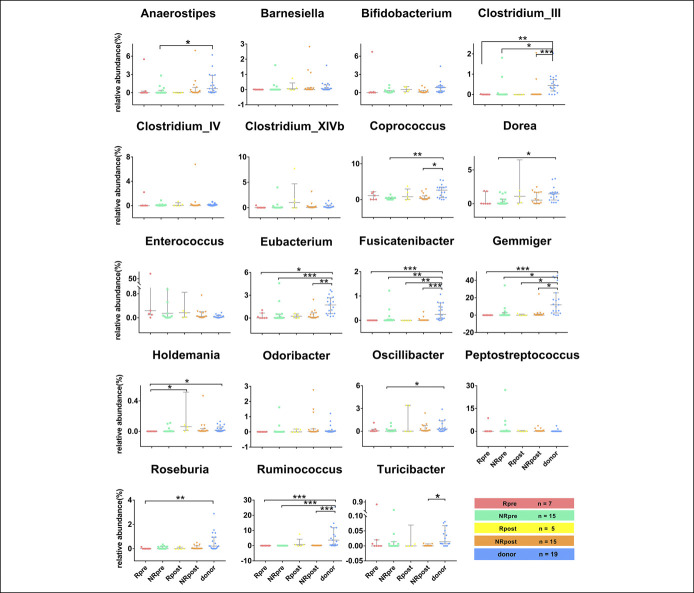
Results: The median maintaining time of the efficacy was 120 days (IQR, 45-180) and 182.5 days (IQR, 105-311.25) from the first course and second course of FMT, respectively. No FMT-related serious adverse events were observed. The differences of the relative abundance in Eggerthella, Lactobacillus, and Ruminococcus between pre-FMT and 5 days post-FMT were remarkably correlated with the long-term clinical remission (P < 0.05).
Discussion: This study demonstrated that patients with UC should undergo the second course of FMT within 4 months after the first course of FMT for maintaining the long-term clinical benefits. The short-term alterations of microbiota after FMT may be conducive to predicting the long-term efficacy of FMT in UC (see Visual Abstract, Supplementary Digital Content, http://links.lww.com/CTG/A363).
Trial registration: ClinicalTrials.gov NCT01790061.
Conflict of interest statement
Figures
Similar articles
-
Long-term efficacy and safety of monotherapy with a single fresh fecal microbiota transplant for recurrent active ulcerative colitis: a prospective randomized pilot study.Microb Cell Fact. 2021 Jan 19;20(1):18. doi: 10.1186/s12934-021-01513-6. Microb Cell Fact. 2021. PMID: 33468164 Free PMC article. Clinical Trial.
-
Efficacy and safety of single fecal microbiota transplantation for Japanese patients with mild to moderately active ulcerative colitis.J Gastroenterol. 2017 Apr;52(4):476-482. doi: 10.1007/s00535-016-1271-4. Epub 2016 Oct 11. J Gastroenterol. 2017. PMID: 27730312 Clinical Trial.
-
Effect of Fecal Microbiota Transplantation on 8-Week Remission in Patients With Ulcerative Colitis: A Randomized Clinical Trial.JAMA. 2019 Jan 15;321(2):156-164. doi: 10.1001/jama.2018.20046. JAMA. 2019. PMID: 30644982 Free PMC article. Clinical Trial.
-
[Ulcerative colitis: Does the modulation of gut microbiota induce long-lasting remission?].Z Gastroenterol. 2019 Jul;57(7):834-842. doi: 10.1055/a-0874-6603. Epub 2019 Apr 15. Z Gastroenterol. 2019. PMID: 30986885 Review. German.
-
Fecal microbiota transplantation for ulcerative colitis.Immunol Med. 2021 Mar;44(1):30-34. doi: 10.1080/25785826.2020.1792040. Epub 2020 Jul 14. Immunol Med. 2021. PMID: 32663072 Review.
Cited by
-
Ginsenoside Rg1 Alleviates Acute Ulcerative Colitis by Modulating Gut Microbiota and Microbial Tryptophan Metabolism.Front Immunol. 2022 May 17;13:817600. doi: 10.3389/fimmu.2022.817600. eCollection 2022. Front Immunol. 2022. PMID: 35655785 Free PMC article.
-
Washed Microbiota Transplantation Improves the Sleep Quality in Patients with Inflammatory Bowel Disease.Nat Sci Sleep. 2024 Aug 2;16:1141-1152. doi: 10.2147/NSS.S460882. eCollection 2024. Nat Sci Sleep. 2024. PMID: 39109266 Free PMC article.
-
Fecal Microbiota Transplantation as Therapy for Treatment of Active Ulcerative Colitis: A Systematic Review and Meta-Analysis.Gastroenterol Res Pract. 2021 Apr 23;2021:6612970. doi: 10.1155/2021/6612970. eCollection 2021. Gastroenterol Res Pract. 2021. PMID: 33981340 Free PMC article. Review.
-
The Role of Fecal Microbiota Transplantation in the Treatment of Inflammatory Bowel Disease.J Clin Med. 2021 Sep 8;10(18):4055. doi: 10.3390/jcm10184055. J Clin Med. 2021. PMID: 34575166 Free PMC article. Review.
-
An Immunologic Compatibility Testing Was Not Useful for Donor Selection in Fecal Microbiota Transplantation for Ulcerative Colitis.Front Immunol. 2021 Jun 4;12:683387. doi: 10.3389/fimmu.2021.683387. eCollection 2021. Front Immunol. 2021. PMID: 34149723 Free PMC article.
References
-
- Ordas I, Eckmann L, Talamini M, et al. Ulcerative colitis. Lancet 2012;380(9853):1606–19. - PubMed
-
- Caruso R, Lo BC, Nunez G. Host-microbiota interactions in inflammatory bowel disease. Nat Rev Immunol 2020;20(7):411–426. - PubMed
-
- Xavier RJ, Podolsky DK. Unravelling the pathogenesis of inflammatory bowel disease. Nature 2007;448(7152):427–34. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
