

Efficacy of Norfloxacin Prophylaxis to Prevent Spontaneous Bacterial Peritonitis: A Systematic Review and Meta-Analysis
- PMID: 32955202
- PMCID: PMC7431273
- DOI: 10.14309/ctg.0000000000000223
Efficacy of Norfloxacin Prophylaxis to Prevent Spontaneous Bacterial Peritonitis: A Systematic Review and Meta-Analysis
Abstract
Introduction: With the emergence of multidrug-resistant organisms, the efficacy of antibiotic prophylaxis to prevent spontaneous bacterial peritonitis (SBP) has been debated. The aim of this study was to assess factors impacting effectiveness of SBP prophylaxis.
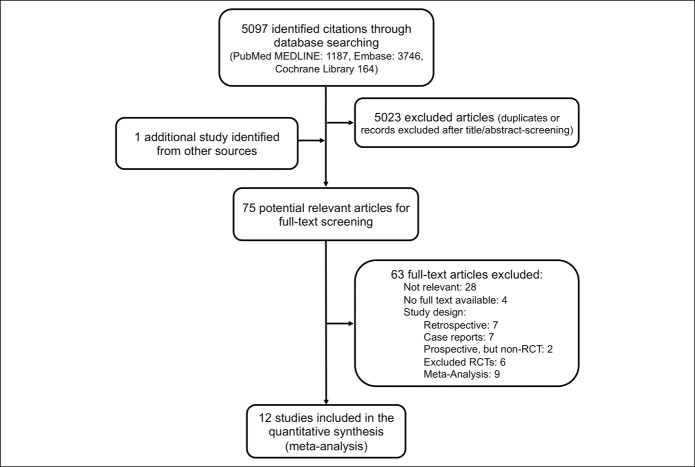
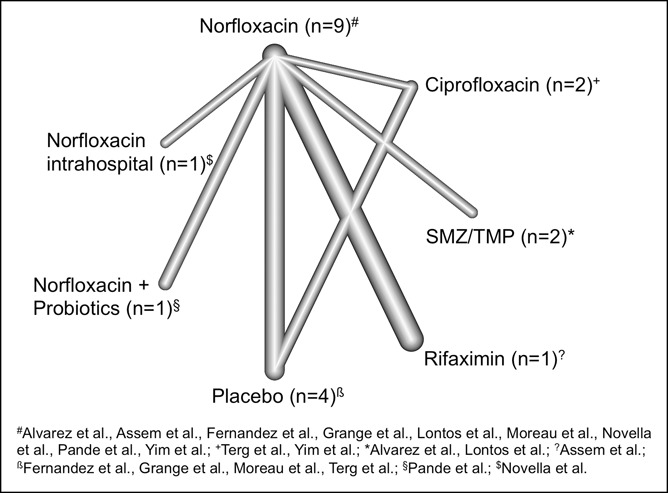
Methods: We searched PubMed, Embase, and the Cochrane Registry from inception to May 2019 to identify randomized controlled trials of patients with liver cirrhosis that assessed SBP occurrence/recurrence during antibiotic prophylaxis with the common antibiotic agents. Network meta-analysis was performed, pooling data with regard to incidence rate ratios (IRRs) of SBP, death, or extraperitoneal infections.
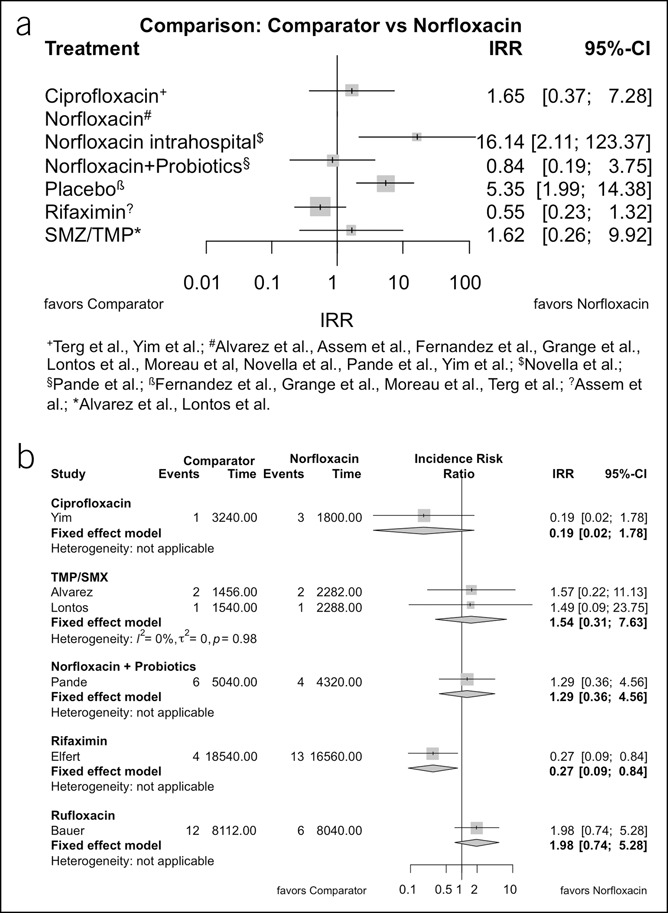
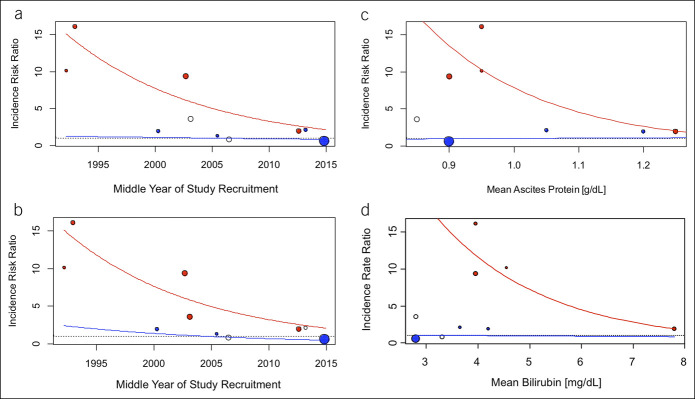
Results: Overall, 1,626 patients in 12 randomized controlled trials were included. During primary prophylaxis, the incidence rate of SBP and death in the norfloxacin-treated patients was 0.117 and 0.438 per patient-year, respectively, and IRRs of placebo vs norfloxacin were significantly higher (IRR 5.35, 95% confidence interval 1.99-14.38, P = 0.0009 for SBP and IRR 2.04, 95% confidence interval 1.20-3.44, P = 0.008 for death). The efficacy of norfloxacin to prevent SBP, but not death, decreased over time (annual percent change from 1992 to 2015 8.2%, P = 0.019), The positive treatment effect was lower in studies including patients with increased ascites protein (P = 0.021) or exceedingly high serum bilirubin (P = 0.012) levels. Norfloxacin was not superior to other antibiotics. The incidence rate of SBP was 2.5-fold higher in patients treated with norfloxacin as secondary compared with primary prophylaxis. No significant differences between treatment designs were observed in secondary prophylaxis.
Discussion: Norfloxacin remained superior to placebo in preventing SBP, yet the efficacy to prevent SBP, not death, decreased over time. Further studies to understand this phenomenon are urgently needed.
Conflict of interest statement
Figures
Comment in
-
A New Window to Favorable Outcome in Acute-on-Chronic Liver Failure.Am J Gastroenterol. 2022 May 1;117(5):815. doi: 10.14309/ajg.0000000000001703. Epub 2022 Mar 18. Am J Gastroenterol. 2022. PMID: 35311796 No abstract available.
-
Response to Mir et al.Am J Gastroenterol. 2022 May 1;117(5):816. doi: 10.14309/ajg.0000000000001760. Am J Gastroenterol. 2022. PMID: 35501977 No abstract available.
References
-
- Arvaniti V, D'Amico G, Fede G, et al. Infections in patients with cirrhosis increase mortality four-fold and should be used in determining prognosis. Gastroenterology 2010;139(4):1246–5, 1256 e1-5. - PubMed
-
- Bernard B, Grangé JD, Khac EN, et al. Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: A meta-analysis. Hepatology 1999;29(6):1655–61. - PubMed
-
- Tito L, Rimola A, Gines P, et al. Recurrence of spontaneous bacterial peritonitis in cirrhosis: Frequency and predictive factors. Hepatology 1988;8(1):27–31. - PubMed
-
- Mücke MM, Rumyantseva T, Mücke VT, et al. Bacterial infection-triggered acute-on-chronic liver failure is associated with increased mortality. Liver Int 2018;38(4):645–53. - PubMed
-
- Wiest R, Lawson M, Geuking M. Pathological bacterial translocation in liver cirrhosis. J Hepatol 2014;60(1):197–209. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
