

Induction and characterization of pancreatic cancer in a transgenic pig model
- PMID: 32956389
- PMCID: PMC7505440
- DOI: 10.1371/journal.pone.0239391
Induction and characterization of pancreatic cancer in a transgenic pig model
Abstract
Background: Preclinical testing of new locoregional therapies for pancreatic cancer has been challenging, due to the lack of a suitable large animal model.
Purpose: To develop and characterize a porcine model of pancreatic cancer. Unlike small animals, pigs have similar physiology, drug dosing, and immune response to humans. Locoregional therapy in pigs can be performed using the same size catheters and devices as in humans.
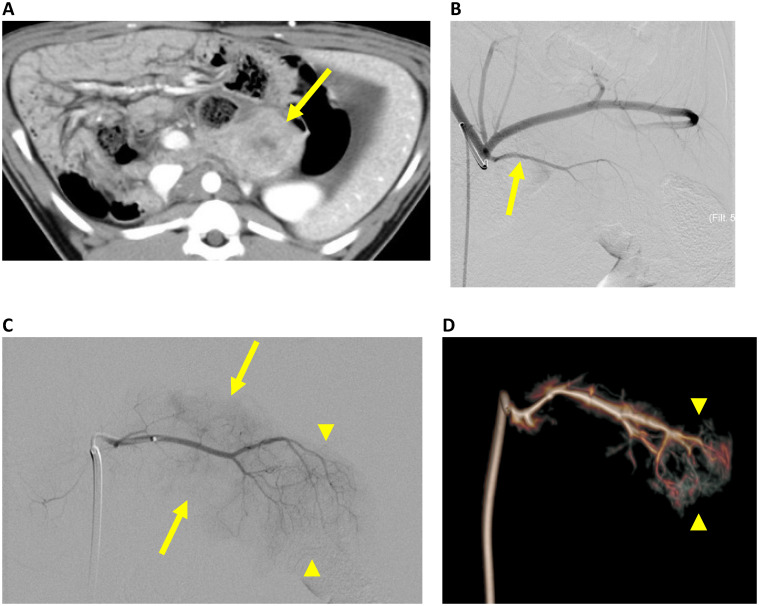
Methods: The Oncopig is a transgenic pig with Cre-inducible TP53R167H and KRASG12D mutations. In 12 Oncopigs, CT-guided core biopsy of the pancreas was performed. The core biopsy was incubated with an adenoviral vector carrying the Cre recombinase gene. The transformed core biopsy was injected back into the pancreas (head, tail, or both). The resulting tumors (n = 19) were characterized on multi-phase contrast-enhanced CT, and on pathology, including immunohistochemistry. Angiographic characterization of the tumors was performed in 3 pigs.
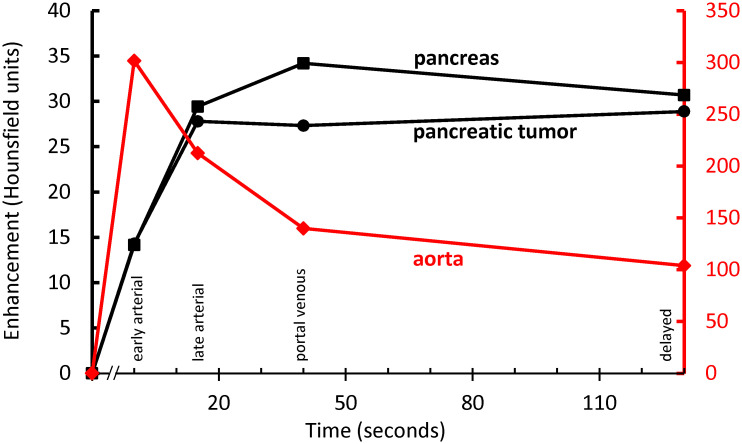
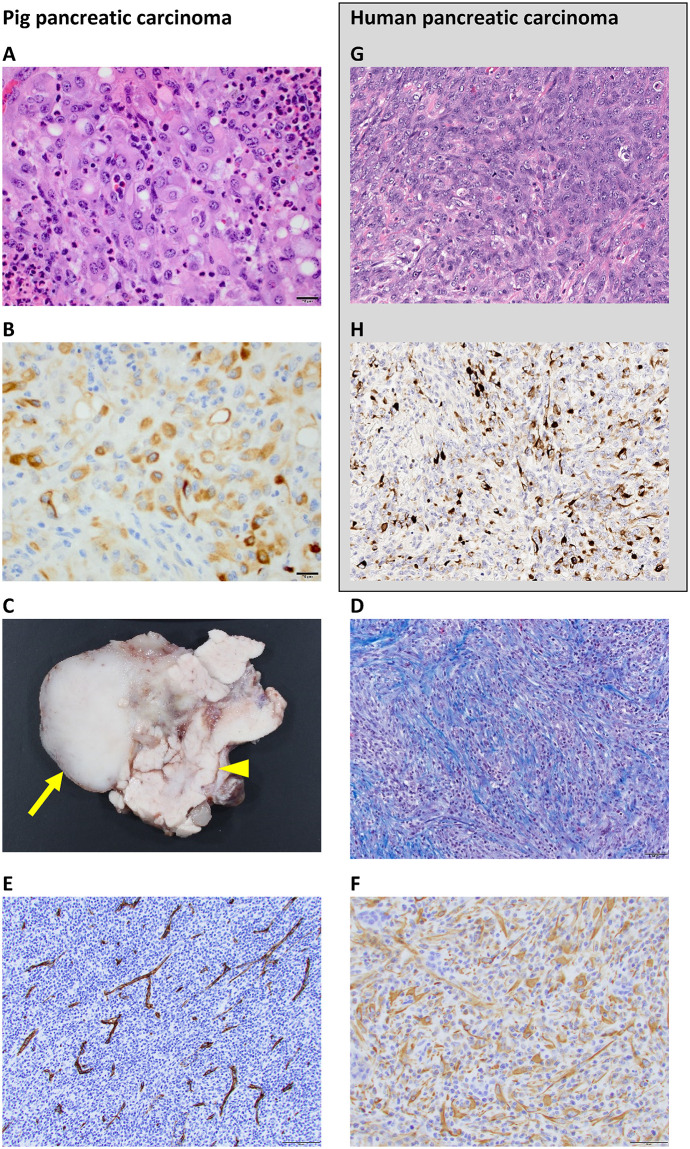
Results: Pancreatic tumors developed at 19 out of 22 sites (86%) that were inoculated. Average tumor size was 3.0 cm at 1 week (range: 0.5-5.1 cm). H&E and immunohistochemical stains revealed undifferentiated carcinomas, similar to those of the pancreatobiliary system in humans. Neoplastic cells were accompanied by a major inflammatory component. 1 of 12 pigs only had inflammatory nodules without evidence of neoplasia. On multiphase CT, tumors were hypovascular compared to the normal pancreas. There was no pancreatic duct dilation. In 3 pigs, angiography was performed, and in all 3 cases, the artery supplying the pancreatic tumor could be catheterized using a 2.4 F microcatheter. Selective angiography showed the pancreatic tumor, without extra-pancreatic perfusion.
Conclusion: Pancreatic cancer can be induced in a transgenic pig. Intra-arterial procedures using catheters designed for human interventions were technically feasible in this large animal model.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: FEB is a co-founder of Claripacs, LLC. He received research funding (investigator-initiated) from Guerbet. He received research support (investigator-initiated) from GE. He received research supplies (investigator-initiated) from Bayer. He received a research grant and speaker fees from Society of Interventional Oncology, which were sponsored by Guerbet. He attended research meetings sponsored by Guerbet. He is an investor in Labdoor, Qventus, CloudMedx, Notable Labs, and Xgenomes. He is the inventor and assignee on US patent 8233586, and is an inventor on US provisional patent applications 62/754,139 and 62/817,116. SBS is a consultant for Johnson & Johnson, Aperture Medical, XACT Robotics, Innoblative, Endoways, and Varian. He received grants from GE Healthcare, AngioDynamics, Elesta, and Johnson & Johnson. He is a shareholder in Aspire Bariatrics, Aperture Medical, Johnson & Johnson, Immunomedics, Impulse, Motus GI, and Progenics. HY is an advisory board member of Genetech and BD Medical. AS is the inventor of Vascular Targeted Photodynamic Therapy with TOOKAD, licensed by Yeda, the commercial branch of the Weizmann Institute, to Steba Biotech. LBS has an equity consulting role in Sus Clinicals, Inc. The Competing Interests Statement in the manuscript is complete, including: research support from GE, consulting agreements, and patents. None of the authors are employees of GE. GE had no control over study design, data analysis, or the contents of the manuscript. The authors are not aware of any intellectual property owned by GE that is related to the pig pancreatic cancer model presented in this paper.
Figures
References
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–21. Epub 2014/05/21. 10.1158/0008-5472.CAN-14-0155 . - DOI - PubMed
-
- Scheffer HJ, Vroomen LG, de Jong MC, Melenhorst MC, Zonderhuis BM, Daams F, et al. Ablation of Locally Advanced Pancreatic Cancer with Percutaneous Irreversible Electroporation: Results of the Phase I/II PANFIRE Study. Radiology. 2017;282(2):585–97. Epub 2016/09/08. 10.1148/radiol.2016152835 . - DOI - PubMed
-
- Yoon H, Mandel JE, Zener R, Yarmohammadi H, Solomon SB, Sofocleous CT, et al., editors. Outcomes after locoregional therapy of pancreatic adenocarcinoma liver metastases. WCIO; 2018; Boston, MA.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
