

SARS-CoV-2 Seroprevalence among Healthcare, First Response, and Public Safety Personnel, Detroit Metropolitan Area, Michigan, USA, May-June 2020
- PMID: 32956614
- PMCID: PMC7706918
- DOI: 10.3201/eid2612.203764
SARS-CoV-2 Seroprevalence among Healthcare, First Response, and Public Safety Personnel, Detroit Metropolitan Area, Michigan, USA, May-June 2020
Abstract
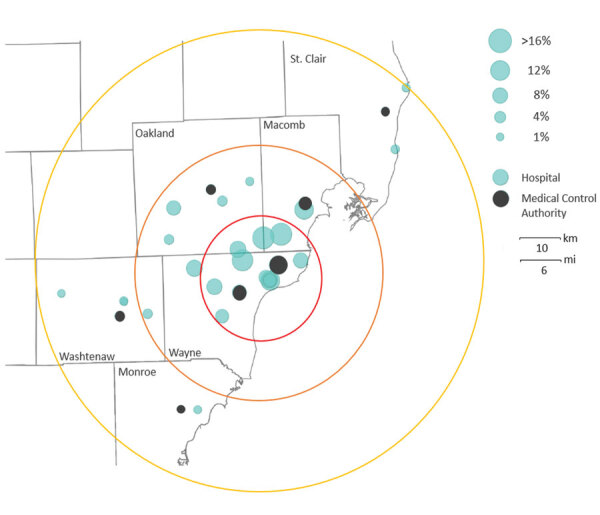
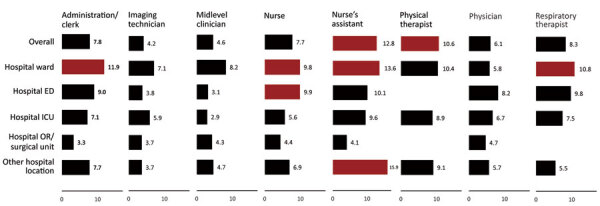
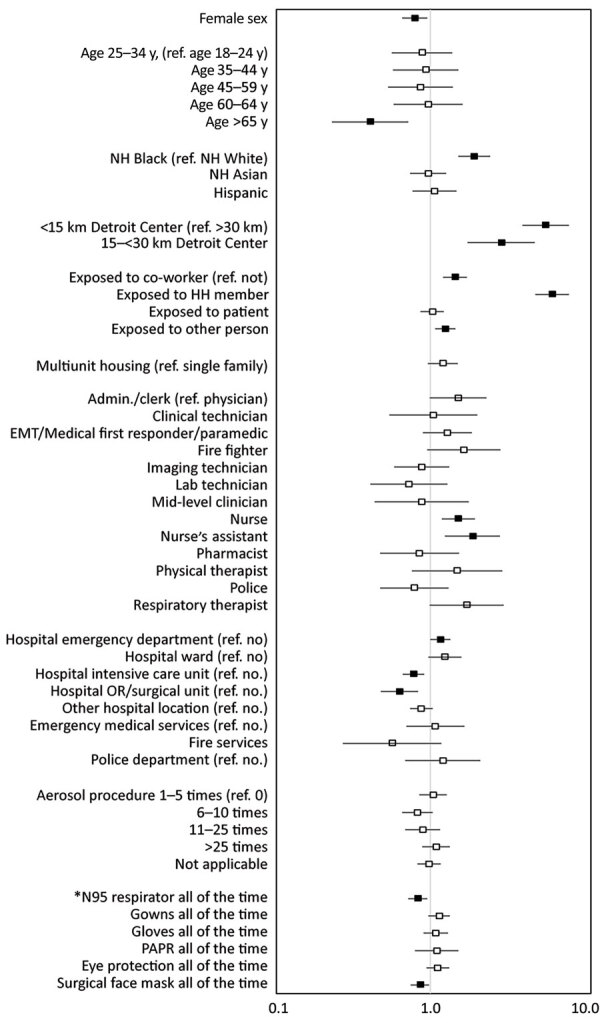
To estimate seroprevalence of severe acute respiratory syndrome 2 (SARS-CoV-2) among healthcare, first response, and public safety personnel, antibody testing was conducted in emergency medical service agencies and 27 hospitals in the Detroit, Michigan, USA, metropolitan area during May-June 2020. Of 16,403 participants, 6.9% had SARS-CoV-2 antibodies. In adjusted analyses, seropositivity was associated with exposure to SARS-CoV-2-positive household members (adjusted odds ratio [aOR] 6.18, 95% CI 4.81-7.93) and working within 15 km of Detroit (aOR 5.60, 95% CI 3.98-7.89). Nurse assistants (aOR 1.88, 95% CI 1.24-2.83) and nurses (aOR 1.52, 95% CI 1.18-1.95) had higher likelihood of seropositivity than physicians. Working in a hospital emergency department increased the likelihood of seropositivity (aOR 1.16, 95% CI 1.002-1.35). Consistently using N95 respirators (aOR 0.83, 95% CI 0.72-0.95) and surgical facemasks (aOR 0.86, 95% CI 0.75-0.98) decreased the likelihood of seropositivity.
Keywords: 2019 novel coronavirus disease; COVID-19; Detroit; SARS-CoV-2; coronavirus disease; emergency responders; hospitals; personal protective equipment; public safety; seroepidemiologic studies; severe acute respiratory syndrome coronavirus 2; viruses; zoonoses.
Figures
References
-
- US Department of Health and Human Services. Title 45 Code of Federal Regulations 46, Protection of human subjects [cited May 1, 2020]. https://www.ecfr.gov/cgi-bin/text-idx?m=08&d=16&y=2020&cd=20200813&submi...
-
- US Food and Drug Administration. EUA authorized serology test performance; 2020. [cited 2020 Jul 30]. https://www.fda.gov/medical-devices/emergency-situations-medical-devices...
-
- National Institute for Occupational Safety and Health. NIOSH industry and occupation computerized coding system (NIOCCS) [cited 2020 Jun 25]. https://www.fda.gov/medical-devices/emergency-situations-medical-devices...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
