

Glioblastoma cell differentiation trajectory predicts the immunotherapy response and overall survival of patients
- PMID: 32957084
- PMCID: PMC7585071
- DOI: 10.18632/aging.103695
Glioblastoma cell differentiation trajectory predicts the immunotherapy response and overall survival of patients
Abstract
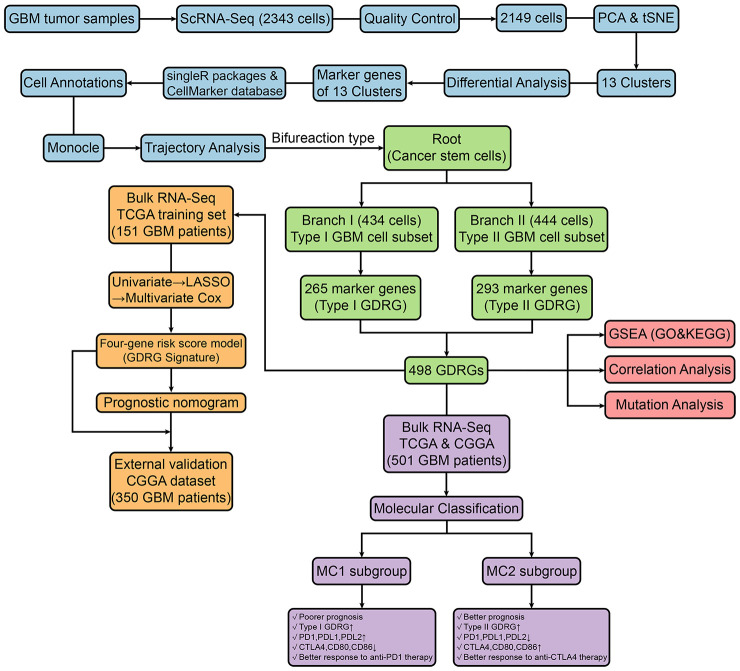
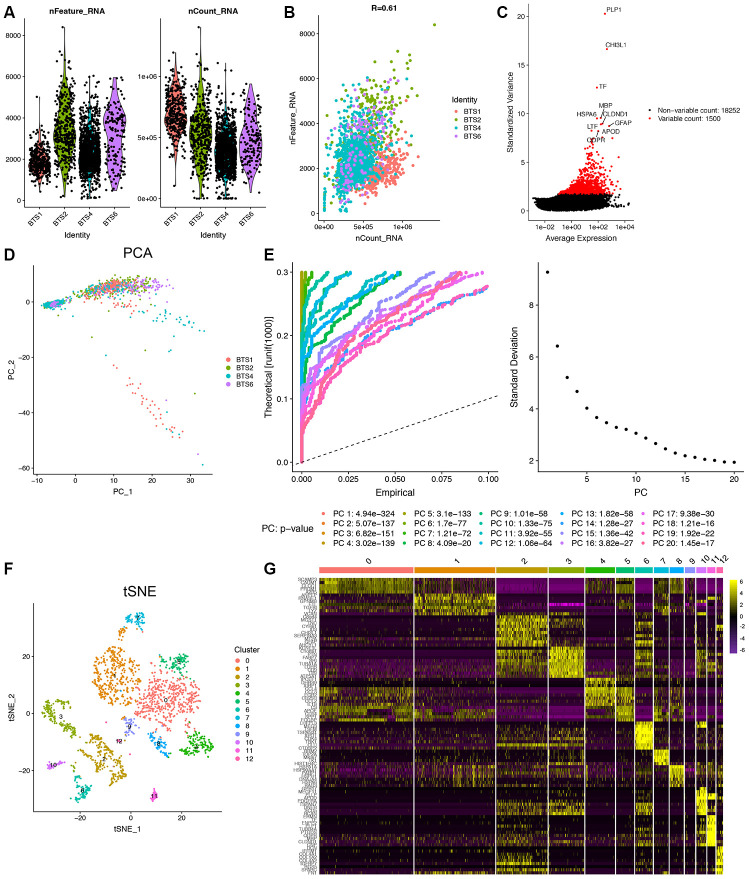
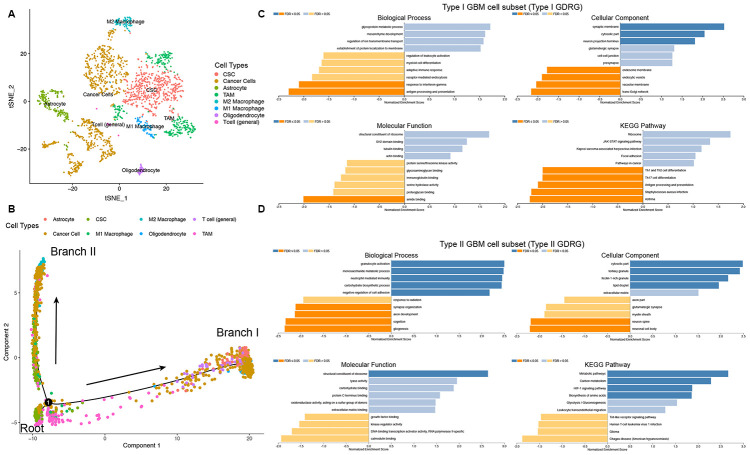
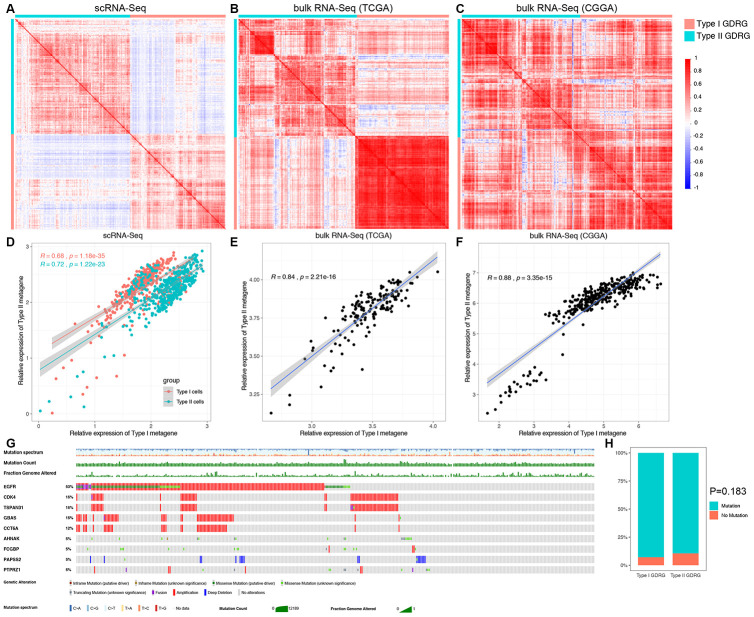
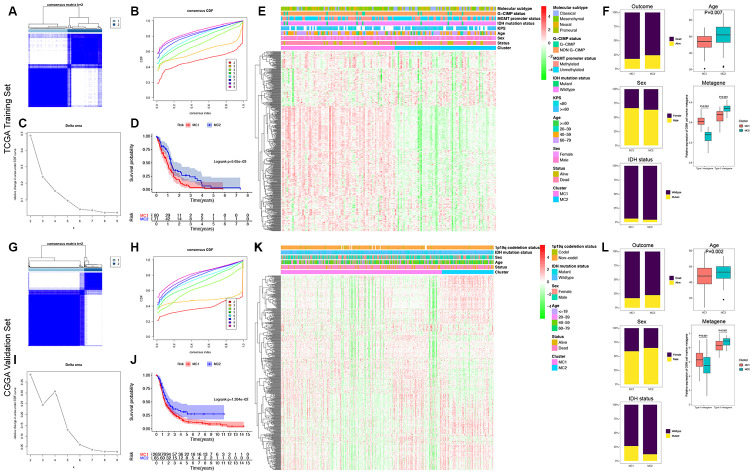
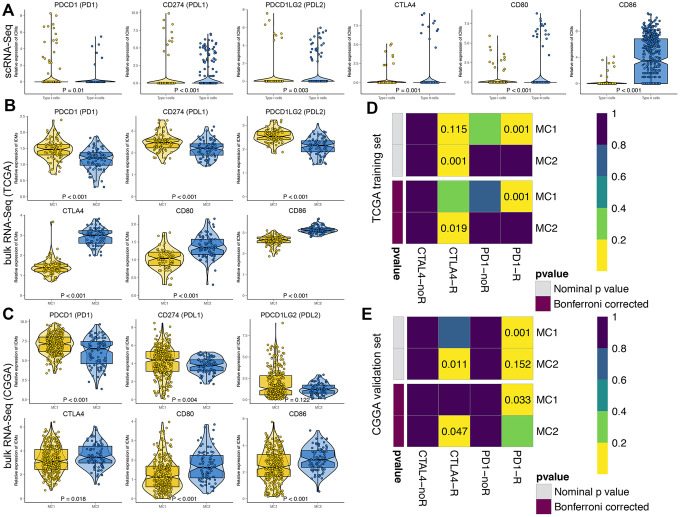
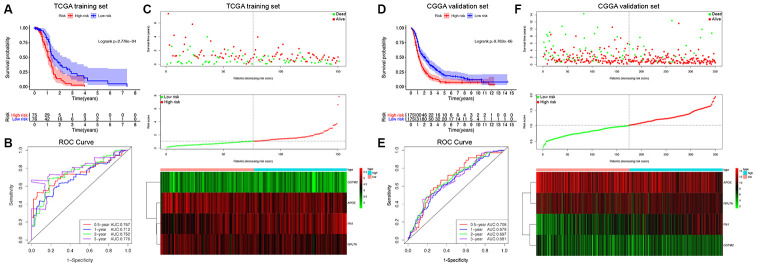
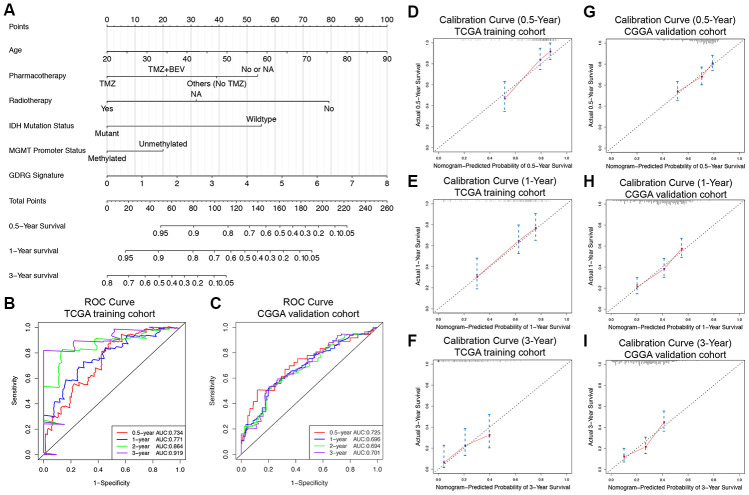
Glioblastoma (GBM) is the most common and lethal primary brain tumor. In this study, we aimed to investigate the differentiation states of GBM cells and their clinical relevance. Integrated single-cell RNA-sequencing (scRNA-seq) data and bulk RNA-seq data from GBM samples were used for analysis. Two subsets of GBM cells in distinct differentiation states were characterized, and 498 GBM cell differentiation-related genes (GDRGs) were identified. GDRGs were significantly correlated with immune regulation and metabolic pathways. We classified the GBM patients into two groups based on the expression of GDRGs in tumors and found that the cell differentiation-based classification successfully predicted patient overall survival (OS), immune checkpoint expression and likelihood of immunotherapy response in GBMs. FN1, APOE, RPL7A and GSTM2 were the 4 most significant survival-predicting GDRGs, and patients with different expression levels of each of these genes had distinct survival outcomes. Finally, a nomogram composed of the GDRG signature, age, pharmacotherapy, radiotherapy, IDH mutations and MGMT promoter methylation was generated and validated in two large GBM cohorts to predict GBM prognosis. This study highlights the significant roles of cell differentiation in predicting the clinical outcomes of GBM patients and their potential response to immunotherapy, suggesting promising therapeutic targets for GBM.
Keywords: cancer cell differentiation; glioblastoma; immunotherapy response; overall survival; trajectory analysis.
Conflict of interest statement
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
