

Laparoscopic procedure is associated with lower morbidity for simultaneous resection of colorectal cancer and liver metastases: an updated meta-analysis
- PMID: 32958079
- PMCID: PMC7507629
- DOI: 10.1186/s12957-020-02018-z
Laparoscopic procedure is associated with lower morbidity for simultaneous resection of colorectal cancer and liver metastases: an updated meta-analysis
Abstract
Background: It has been demonstrated that simultaneous resection of both primary colorectal lesion and metastatic hepatic lesion is a safe approach with low mortality and postoperative complication rates. However, there are some controversies over which kind of surgical approach is better. The aim of study was to compare the efficacy and safety of laparoscopic surgeries and open surgeries for simultaneous resection of colorectal cancer (CRC) and synchronous colorectal liver metastasis (SCRLM).
Methods: A systemic search of online database including PubMed, Web of Science, Cochrane Library, and Embase was performed until June 5, 2019. Intraoperative complications, postoperative complications, and long-term outcomes were synthesized by using STATA, version 15.0. Cumulative and single-arm meta-analyses were also conducted.
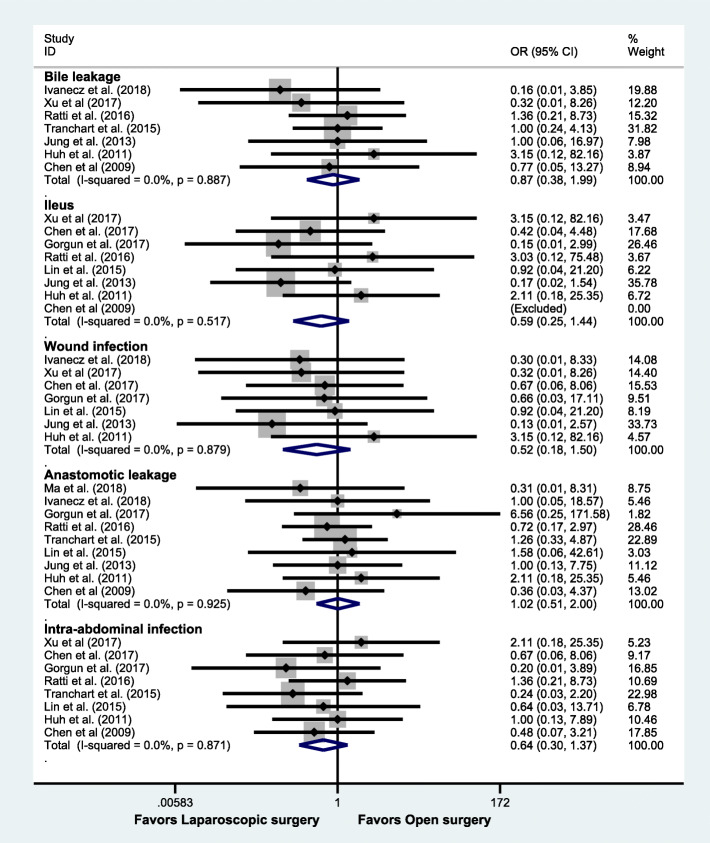
Results: It contained twelve studies with 616 patients (273 vs 343, laparoscopic surgery group and open surgery group, respectively) and manifested latest surgical results for the treatment of CRC and SCRLM. Among patients who underwent laparoscopic surgeries, they had lower rates of postoperative complications (OR = 0.66, 95% CI: 0.46 to 0.96, P = 0.028), less intraoperative blood loss (weight mean difference (WMD) = - 113.31, 95% CI: - 189.03 to - 37.59, P = 0.003), less time in the hospital and recovering after surgeries (WMD = - 2.70, 95% CI: - 3.99 to - 1.40, P = 0.000; WMD = - 3.20, 95% CI: - 5.06 to - 1.34, P = 0.001), but more operating time (WMD = 36.57, 95% CI: 7.80 to 65.35, P = 0.013). Additionally, there were no statistical significance between two kinds of surgical approaches in disease-free survival and overall survival. Moreover, cumulative meta-analysis indicated statistical difference in favor of laparoscopic surgery in terms of morbidity was firstly detected in the 12th study in 2018 (OR = 0.66, 95% CI: 0.46 to 0.96, P = 0.028) as the 95% CI narrowed.
Conclusion: Compared with open surgeries, laparoscopic surgeries are safer (postoperative complications and intraoperative blood loss) and more effective (length of hospital stay and postoperative stay), and it can be considered as the first option for management of SCRLM in high-volume laparoscopic centers.
Trial registration: CRD42020151176.
Keywords: Colorectal cancer; Laparoscopy; Meta-analysis; Synchronous liver metastasis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA: A Cancer Journal for Clinicians. 2019;69:7–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
