

Study protocol for an observational study of cerebrospinal fluid pressure in patients with degenerative cervical myelopathy undergoing surgical deCOMPression of the spinal CORD: the COMP-CORD study
- PMID: 32958488
- PMCID: PMC7507854
- DOI: 10.1136/bmjopen-2020-037332
Study protocol for an observational study of cerebrospinal fluid pressure in patients with degenerative cervical myelopathy undergoing surgical deCOMPression of the spinal CORD: the COMP-CORD study
Abstract
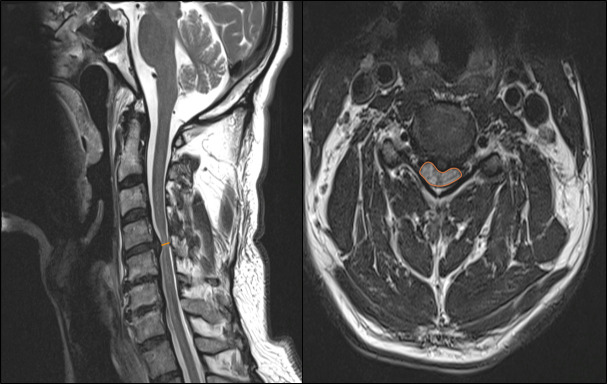
Introduction: Degenerative cervical myelopathy (DCM) is a disabling spinal disorder characterised by sensorimotor deficits of upper and lower limbs, neurogenic bladder dysfunction and neuropathic pain. When suspected, cervical MRI helps to reveal spinal cord compression and rules out alternative diagnoses. However, the correlation between radiological findings and symptoms is weak. Cerebrospinal fluid pressure (CSFP) analysis may complement the appreciation of cord compression and be used for intraoperative and postoperative monitorings in patients undergoing surgical decompression.
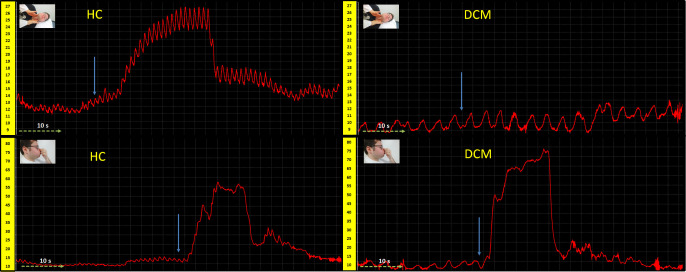
Methods and analysis: Twenty patients diagnosed with DCM undergoing surgical decompression will receive standardised lumbar CSFP monitoring immediately before, during and 24 hours after operation. Rest (ie, opening pressure, CSF pulsation) and stimulated (ie, Valsalva, Queckenstedt's) CSFP-findings in DCM will be compared with 20 controls and results from CSFP monitoring will be related to clinical and neurophysiological findings. Arterial blood pressure will be recorded perioperatively and postoperatively to calculate spinal cord perfusion pressure and spinal vascular reactivity index. Furthermore, measures of CSFP will be compared with markers of spinal cord compression by means of MR imaging.
Ethics and dissemination: The study protocol conformed to the latest revision of the Declaration of Helsinki and was approved by the local Ethics Committee of the University Hospital of Zurich (KEK-ZH number PB-2016-00623). The main publications from this study will cover the CSFP fluid dynamics and pressure analysis preoperative, perioperative and postoperative correlated with imaging, clinical scores and neurophysiology. Other publications will deal with preoperative and postoperative spinal perfusion. Furthermore, we will disseminate an analysis on waveform morphology and the correlation with blood pressure and ECG. Parts of the data will be used for computational modelling of cervical stenosis.
Trial registration number: ClinicalTrials.gov Registry (NCT02170155).
Keywords: adult neurology; neurophysiology; neurosurgery; spine.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Intraoperative Monitoring of CSF Pressure in Patients with Degenerative Cervical Myelopathy (COMP-CORD Study): A Prospective Cohort Study.J Neurotrauma. 2022 Feb;39(3-4):300-310. doi: 10.1089/neu.2021.0310. J Neurotrauma. 2022. PMID: 34806912
-
Safety and Feasibility of Lumbar Cerebrospinal Fluid Pressure and Intraspinal Pressure Studies in Cervical Stenosis: A Case Series.Acta Neurochir Suppl. 2021;131:367-372. doi: 10.1007/978-3-030-59436-7_70. Acta Neurochir Suppl. 2021. PMID: 33839876
-
Cerebrospinal Fluid Pressure Dynamics as a Bedside Test in Traumatic Spinal Cord Injury to Assess Surgical Spinal Cord Decompression: Safety, Feasibility, and Proof-of-Concept.Neurorehabil Neural Repair. 2023 Apr;37(4):171-182. doi: 10.1177/15459683231159662. Epub 2023 Mar 15. Neurorehabil Neural Repair. 2023. PMID: 36919616 Free PMC article.
-
Cerebrospinal fluid pressure dynamics as a biomechanical marker for quantification of spinal cord compression: Conceptual framework and systematic review of clinical trials.Brain Spine. 2025 Feb 12;5:104211. doi: 10.1016/j.bas.2025.104211. eCollection 2025. Brain Spine. 2025. PMID: 40041396 Free PMC article. Review.
-
The rise and fall of Queckenstedt's test between 1916 and 1970, a milestone in spinal cord diagnostics and why it matters.Eur J Neurol. 2025 Jan;32(1):e16556. doi: 10.1111/ene.16556. Epub 2024 Nov 27. Eur J Neurol. 2025. PMID: 39601454 Free PMC article.
Cited by
-
Medical Communication Services after Traumatic Spinal Cord Injury.J Healthc Eng. 2021 Aug 31;2021:4798927. doi: 10.1155/2021/4798927. eCollection 2021. J Healthc Eng. 2021. Retraction in: J Healthc Eng. 2023 Nov 1;2023:9764817. doi: 10.1155/2023/9764817. PMID: 34512936 Free PMC article. Retracted. Review.
-
Queckenstedt's test repurposed for the quantitative assessment of the cerebrospinal fluid pulsatility curve.Acta Neurochir (Wien). 2023 Jun;165(6):1533-1543. doi: 10.1007/s00701-023-05583-w. Epub 2023 Apr 20. Acta Neurochir (Wien). 2023. PMID: 37079108 Free PMC article.
-
Epidural pressure measurement using a fiber-optic sensor (proof-of-principle in vivo animal trial).Animal Model Exp Med. 2024 Oct;7(5):769-776. doi: 10.1002/ame2.12469. Epub 2024 Jul 9. Animal Model Exp Med. 2024. PMID: 38981680 Free PMC article.
-
A New Framework for Investigating the Biological Basis of Degenerative Cervical Myelopathy [AO Spine RECODE-DCM Research Priority Number 5]: Mechanical Stress, Vulnerability and Time.Global Spine J. 2022 Feb;12(1_suppl):78S-96S. doi: 10.1177/21925682211057546. Global Spine J. 2022. PMID: 35174728 Free PMC article.
-
Intra-, Epidural And Intracranial Pressure Changes During Interlaminar Endoscopy, With and Without Dural Tear.Neurospine. 2025 Jun;22(2):583-591. doi: 10.14245/ns.2550456.228. Epub 2025 Jun 30. Neurospine. 2025. PMID: 40625018 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous