

The impact of hypertonic saline on cerebrovascular reactivity and compensatory reserve in traumatic brain injury: an exploratory analysis
- PMID: 32959342
- PMCID: PMC7505542
- DOI: 10.1007/s00701-020-04579-0
The impact of hypertonic saline on cerebrovascular reactivity and compensatory reserve in traumatic brain injury: an exploratory analysis
Abstract
Background: Intravenous hypertonic saline is utilized commonly in critical care for treatment of acute or refractory elevations of intracranial pressure (ICP) in traumatic brain injury (TBI) patients. Though there is a clear understanding of the general physiological effects of a hypertonic saline solution over long periods of time, smaller epoch effects of hypertonic saline (HTS) have not been thoroughly analyzed. The aim of this study was to perform a direct evaluation of the high-frequency response of HTS on the cerebrovascular physiological responses in TBI.
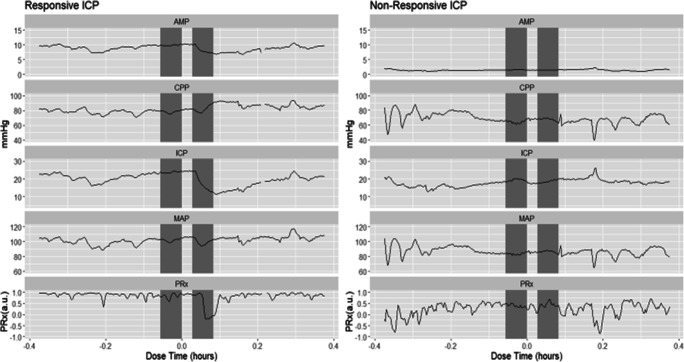
Methods: We retrospectively reviewed our prospectively maintained adult TBI database for those with archived high-frequency cerebral physiology and available HTS treatment information. We evaluated different epochs of physiology around HTS bolus dosing, comparing pre- with post-HTS. We assessed for changes in slow fluctuations in ICP, pulse amplitude of ICP (AMP), cerebral perfusion pressure (CPP), mean arterial pressure (MAP), cerebrovascular reactivity (as measured through pressure reactivity index (PRx)), and cerebral compensatory reserve (correlation (R) between AMP (A) and ICP (P)). Comparisons of mean measures and percentage time above clinically relevant thresholds for the physiological parameters were compared pre- and post-HTS using descriptive statistics and Mann-Whitney U testing. We assessed for subgroups of physiological responses using latent profile analysis (LPA).
Results: Fifteen patients underwent 69 distinct bolus infusions of hypertonic saline. Apart from the well-documented decrease in ICP, there was also a reduction in AMP. The analysis of cerebrovascular reactivity response to HTS solution had two main effects. For patients with grossly impaired cerebrovascular reactivity pre-HTS (PRx > + 0.30), HTS bolus led to improved reactivity. However, for those with intact cerebrovascular reactivity pre-HTS (PRx < 0), HTS bolus demonstrated a trend towards more impaired reactivity. This indicates that HTS has different impacts, dependent on pre-bolus cerebrovascular status. There was no significant change in metrics of cerebral compensatory reserve. LPA failed to demonstrate any subgroups of physiological responses to HTS administration.
Conclusions: The direct decrease in ICP and AMP confirms that a bolus dose of a HTS solution is an effective therapeutic agent for intracranial hypertension. However, in patients with intact autoregulation, hypertonic saline may impair cerebral hemodynamics. These findings regarding cerebrovascular reactivity remain preliminary and require further investigation.
Keywords: Cerebrovascular circulation; Cerebrovascular response; Hypertonic saline; Intracranial pressure; Pressure reactivity index; Sodium chloride.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Equimolar doses of hypertonic agents (saline or mannitol) in the treatment of intracranial hypertension after severe traumatic brain injury.Medicine (Baltimore). 2020 Sep 18;99(38):e22004. doi: 10.1097/MD.0000000000022004. Medicine (Baltimore). 2020. PMID: 32957318 Free PMC article. Clinical Trial.
-
Hypertonic Saline is Superior to Mannitol for the Combined Effect on Intracranial Pressure and Cerebral Perfusion Pressure Burdens in Patients With Severe Traumatic Brain Injury.Neurosurgery. 2020 Feb 1;86(2):221-230. doi: 10.1093/neuros/nyz046. Neurosurgery. 2020. PMID: 30877299 Free PMC article.
-
Post-traumatic multimodal brain monitoring: response to hypertonic saline.J Neurotrauma. 2014 Nov 15;31(22):1872-80. doi: 10.1089/neu.2014.3376. Epub 2014 Sep 11. J Neurotrauma. 2014. PMID: 24915462 Clinical Trial.
-
Hypertonic saline versus other intracranial pressure-lowering agents for people with acute traumatic brain injury.Cochrane Database Syst Rev. 2019 Dec 30;12(12):CD010904. doi: 10.1002/14651858.CD010904.pub2. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2020 Jan 17;1:CD010904. doi: 10.1002/14651858.CD010904.pub3. PMID: 31886900 Free PMC article. Updated.
-
Hypertonic saline versus other intracranial pressure-lowering agents for people with acute traumatic brain injury.Cochrane Database Syst Rev. 2020 Jan 17;1(1):CD010904. doi: 10.1002/14651858.CD010904.pub3. Cochrane Database Syst Rev. 2020. PMID: 31978260 Free PMC article.
Cited by
-
Approaches to neuroprotection in pediatric neurocritical care.World J Crit Care Med. 2023 Jun 9;12(3):116-129. doi: 10.5492/wjccm.v12.i3.116. eCollection 2023 Jun 9. World J Crit Care Med. 2023. PMID: 37397588 Free PMC article. Review.
-
Physiologic Characteristics of Hyperosmolar Therapy After Pediatric Traumatic Brain Injury.Front Neurol. 2021 Apr 20;12:662089. doi: 10.3389/fneur.2021.662089. eCollection 2021. Front Neurol. 2021. PMID: 33959090 Free PMC article.
-
Dynamic Temporal Relationship Between Autonomic Function and Cerebrovascular Reactivity in Moderate/Severe Traumatic Brain Injury.Front Netw Physiol. 2022 Feb 16;2:837860. doi: 10.3389/fnetp.2022.837860. eCollection 2022. Front Netw Physiol. 2022. PMID: 36926091 Free PMC article.
-
Computer Vision for Continuous Bedside Pharmacological Data Extraction: A Novel Application of Artificial Intelligence for Clinical Data Recording and Biomedical Research.Front Big Data. 2021 Aug 27;4:689358. doi: 10.3389/fdata.2021.689358. eCollection 2021. Front Big Data. 2021. PMID: 34514379 Free PMC article.
-
Cerebrovascular Reactivity Is Not Associated With Therapeutic Intensity in Adult Traumatic Brain Injury: A Validation Study.Neurotrauma Rep. 2023 May 12;4(1):307-317. doi: 10.1089/neur.2023.0011. eCollection 2023. Neurotrauma Rep. 2023. PMID: 37187506 Free PMC article.
References
-
- Adams H, Donnelly J, Czosnyka M, Kolias AG, Helmy A, Menon DK, Smielewski P, Hutchinson PJ. Temporal profile of intracranial pressure and cerebrovascular reactivity in severe traumatic brain injury and association with fatal outcome: an observational study. PLoS Med. 2017;14(7):e1002353. doi: 10.1371/journal.pmed.1002353. - DOI - PMC - PubMed
-
- AIR M, Menon DK, Steyerberg EW, Citerio G, Lecky F, Manley GT, Hill S, Legrand V, Sorgner A, CENTER-TBI Participants and Investigators Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI): a prospective longitudinal observational study. Neurosurgery. 2015;76(1):67–80. doi: 10.1227/NEU.0000000000000575. - DOI - PubMed
-
- Bennis FC, Teeuwen B, Zeiler FA, Elting JW, van der Naalt J, Bonizzi P, Delhaas T, Aries MJ (2020) Improving prediction of favourable outcome after 6 months in patients with severe traumatic brain injury using physiological cerebral parameters in a multivariable logistic regression model. Neurocrit Care. 10.1007/s12028-020-00930-6 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
