

Association Between Pain, Blood Pressure, and Medication Intensification in Primary Care: an Observational Study
- PMID: 32959353
- PMCID: PMC7728880
- DOI: 10.1007/s11606-020-06208-z
Association Between Pain, Blood Pressure, and Medication Intensification in Primary Care: an Observational Study
Abstract
Background: Treating hypertension is important but physicians often do not intensify blood pressure (BP) treatment in the setting of pain.
Objective: To identify whether reporting pain is associated with (1) elevated BP at the same visit, (2) medication intensification, and (3) elevated BP at the subsequent visit.
Design: Retrospective cohort SETTING: Integrated health system PARTICIPANTS: Adults seen in primary care EXPOSURE: Pain status based on numerical scale: mild (1-3), moderate (4-6), or severe (≥ 7).
Main measures: We defined elevated BP as ≥ 140/80 mmHg and medication intensification as increasing the dose or adding a new antihypertensive medication. Multilevel regression models were used to find the association between pain and (1) elevated BP at the index visit; (2) medication intensification at the index visit; and (3) elevated BP at the subsequent visit. Models adjusted for demographics, chronic conditions, and clustering within physician. In the third model, we adjusted for initial systolic BP as well.
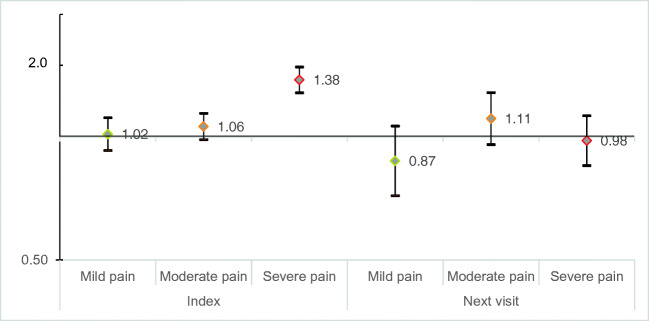
Key results: Our population included 56,322 patients; 3155 (6%) reported mild pain, 5050 (9%) reported moderate pain, and 4647 (8%) reported severe pain at the index visit. Compared with no pain, the adjusted odds ratios of elevated BP were 1.38 (95% CI: 1.28-1.48) for severe pain, 1.06 (95% CI: 0.99-1.14) for moderate pain, and 1.02 (95% CI: 0.93-1.12) for mild pain. Adjusted odds ratios of medication intensification at the index visit were 0.65 (95% CI: 0.54-0.80) for mild pain, 0.61 (95% CI: 0.52-0.72) for moderate pain, and 0.55 (95% CI: 0.47-0.64) for severe pain. Among patients with elevated BP at the index visit, reporting pain at the index visit was not associated with elevated BP at the subsequent visit.
Conclusions: When patients reported pain, physicians were less likely to intensify antihypertensive treatment; nevertheless, patients reporting pain were not more likely to have elevated BP at the subsequent visit.
Keywords: hypertension; medications; pain; primary care; quality of care.
Conflict of interest statement
Dr. Pfoh’s time is supported in part by a National Institute of Health Loan Repayment Grant from the National Heart, Lung, and Blood Institute. All authors report that they have no relevant conflicts of interest to disclose.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
