

Prehabilitation in elective abdominal cancer surgery in older patients: systematic review and meta-analysis
- PMID: 32959532
- PMCID: PMC7709363
- DOI: 10.1002/bjs5.50347
Prehabilitation in elective abdominal cancer surgery in older patients: systematic review and meta-analysis
Abstract
Background: Prehabilitation has emerged as a strategy to prepare patients for elective abdominal cancer surgery with documented improvements in postoperative outcomes. The aim of this study was to assess the evidence for prehabilitation interventions of relevance to the older adult.
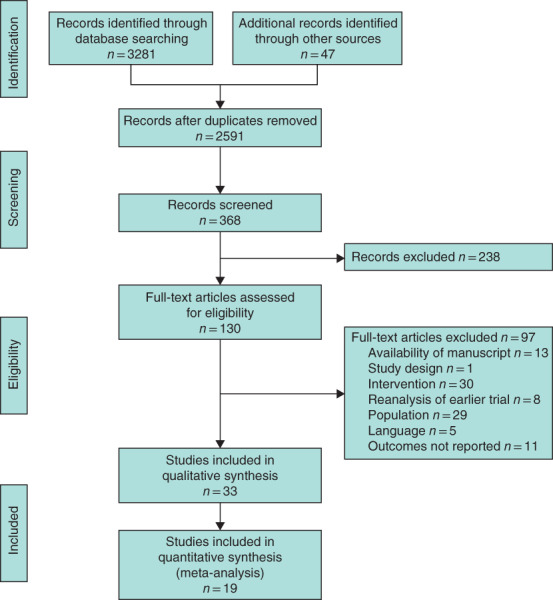
Methods: Systematic searches were conducted using MEDLINE, Web of Science, Scopus, CINAHL and PsychINFO. Studies of preoperative intervention (prehabilitation) in patients undergoing abdominal cancer surgery reporting postoperative outcomes were included. Age limits were not set as preliminary searches revealed this would be too restrictive. Articles were screened and selected based on PRISMA guidelines, and assessment of bias was performed. Qualitative, quantitative and meta-analyses of data were conducted as appropriate.
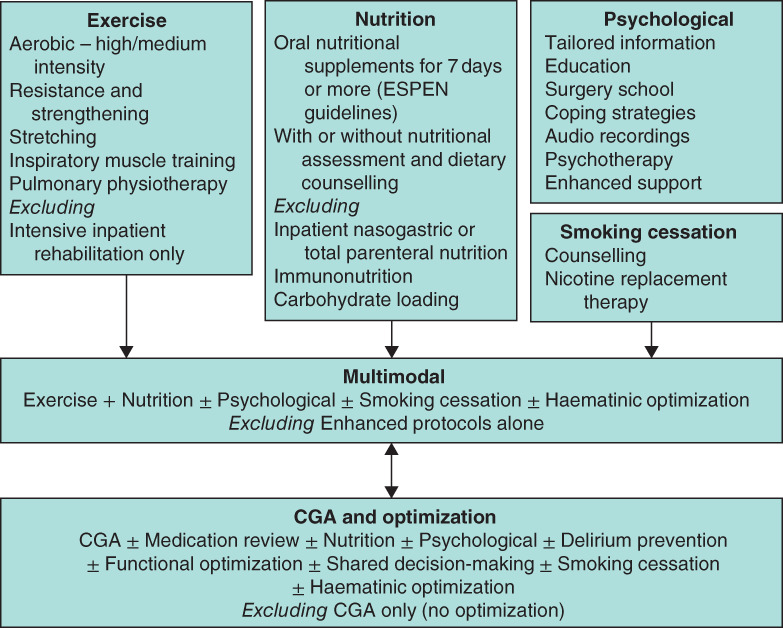
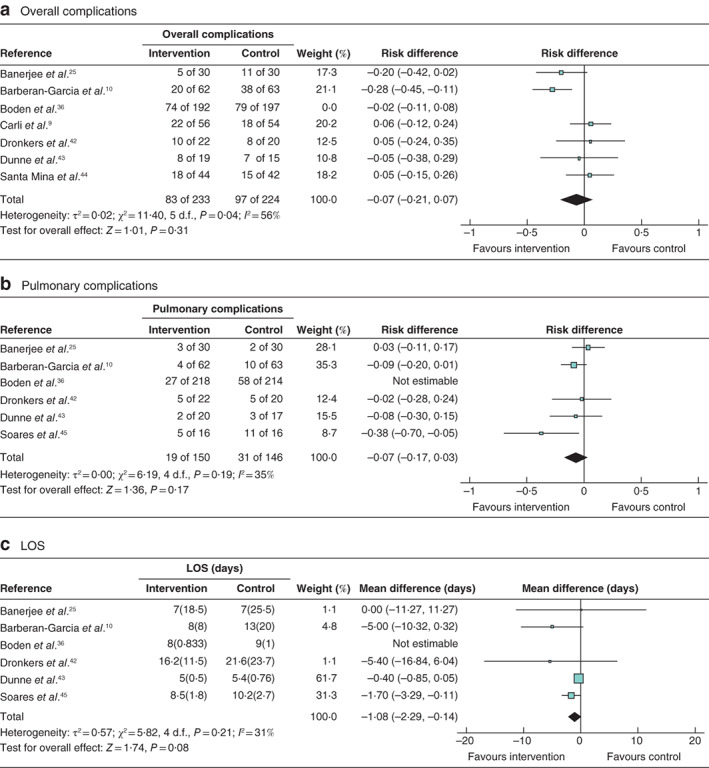
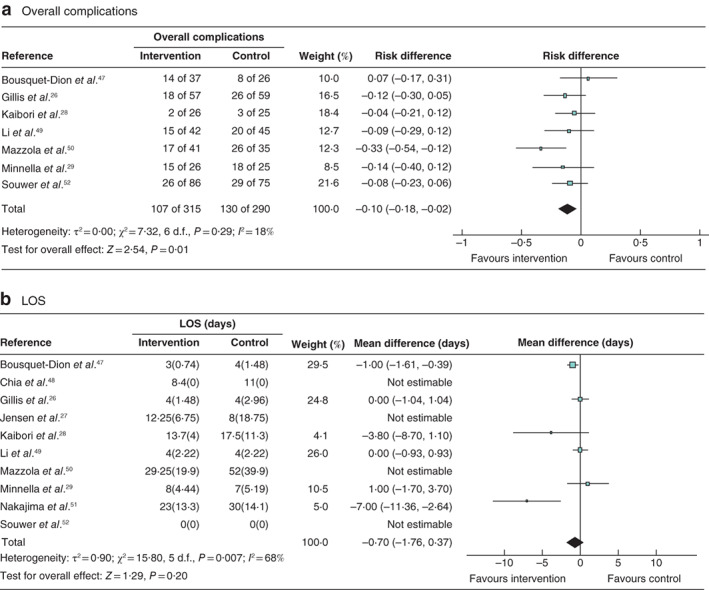
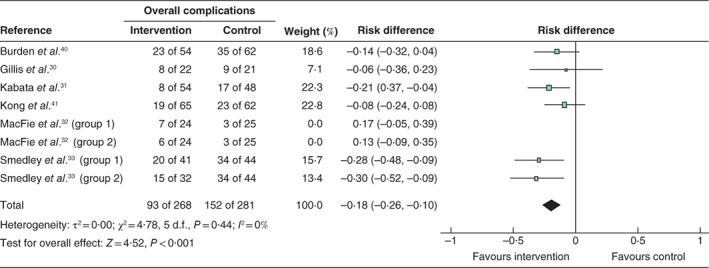
Results: Thirty-three studies (3962 patients) were included. Interventions included exercise, nutrition, psychological input, comprehensive geriatric assessment and optimization, smoking cessation and multimodal (two or more interventions). Nine studies purposely selected high-risk, frail or older patients. Thirty studies were at moderate or high risk of bias. Ten studies individually reported benefits in complication rates, with meta-analyses for overall complications demonstrating significant benefit: multimodal (risk difference -0·1 (95 per cent c.i. -0·18 to -0·02); P = 0·01, I2 = 18 per cent) and nutrition (risk difference -0·18 (-0·26 to -0·10); P < 0·001, I2 = 0 per cent). Seven studies reported reductions in length of hospital stay, with no differences on meta-analysis.
Conclusion: The conclusions of this review are limited by the quality of the included studies, and the heterogeneity of interventions and outcome measures reported. Exercise, nutritional and multimodal prehabilitation may reduce morbidity after abdominal surgery, but data specific to older patients are sparse.
Antecedentes: La pre-habilitación ha surgido como una estrategia para preparar a los pacientes para la cirugía electiva del cáncer abdominal con mejoras documentadas en los resultados postoperatorios. El objetivo de este estudio fue evaluar la evidencia sobre las intervenciones de pre-habilitación relevantes en adultos de edad avanzada. MÉTODOS: Se realizaron búsquedas sistemáticas utilizando MEDLINE, Web of Science, Scopus, CINAHL y PsychINFO. Registro PROSPERO: CRD42019120381. Se incluyeron estudios de intervención preoperatoria (pre-habilitación) en pacientes sometidos a cirugía oncológica abdominal que describiesen resultados postoperatorios. No se fijaron límites en la edad dado que las búsquedas preliminares revelaron que ello sería demasiado restrictivo. Los artículos fueron examinados y seleccionados en base a las guías PRISMA y se realizó una evaluación del sesgo. Se llevó a cabo un análisis cualitativo, cuantitativo y metaanálisis de los datos según fuese apropiado.
Resultados: Se incluyeron 33 estudios (3.962 patients). Las intervenciones incluyeron ejercicio, nutrición, intervención psicológica, evaluación geriátrica global y optimización, abandono del tabaquismo y multimodal (dos o más intervenciones). Nueve estudios seleccionaron expresamente una población de pacientes de elevado riesgo, frágiles o de edad avanzada. Treinta estudios presentaban un riesgo moderado/alto de sesgo. Diez estudios describieron de forma individual beneficios en las tasas de complicaciones con metaanálisis para las complicaciones globales demostrando un beneficio significativo: multimodal (diferencia de riesgo -0,1 (i.c. del 95% −0,18 a −0,02); P = 0,01, I2 = 18%) e intervención nutricional (diferencia de riesgo −0,18 (i.c. del 95% −0,26 a −0,10); P < 0,001, I2 = 0%). Siete estudios describieron reducciones en la duración de la estancia hospitalaria, sin diferencias en el metaanálisis. CONCLUSIÓN: Las conclusiones de esta revisión están limitadas por la calidad de los estudios incluidos, heterogeneidad de las intervenciones y descripción de las medidas de resultados. Las intervenciones de pre-habilitación de ejercicio, nutricionales y multimodales puede reducir la morbilidad tras cirugía abdominal, pero los datos concretos en pacientes de edad avanzada son escasos.
© 2020 The Authors. BJS Open published by John Wiley & Sons Ltd on behalf of British Journal of Surgery Society.
Figures
References
-
- Office for National Statistics . Cancer Registration Statistics, England: 2016 https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/... [accessed 29 March 2019].
-
- West MA, Lythgoe D, Barben CP, Noble L, Kemp GJ, Jack S et al Cardiopulmonary exercise variables are associated with postoperative morbidity after major colonic surgery: a prospective blinded observational study. Br J Anaesth 2014; 112: 665–671. - PubMed
-
- Audisio RA, Veronesi P, Ferrario L, Cipolla C, Andreoni B, Aapro M. Elective surgery for gastrointestinal tumours in the elderly. Ann Oncol 1997; 8: 317–326. - PubMed
-
- Ross R, Blair SN, Arena R, Church TS, Després JP, Franklin BA et al.; American Heart Association Physical Activity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Council on Cardiovascular and Stroke Nursing; Council on Functional Genomics and Translational Biology; Stroke Council . Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American Heart Association. Circulation 2016; 134: e653–e699. - PubMed
-
- Audisio RA, Papamichael D. Treatment of colorectal cancer in older patients. Nat Rev Gastroenterol Hepatol 2012; 9: 716–725. - PubMed
