

Epidemic Landscape and Forecasting of SARS-CoV-2 in India
- PMID: 32959618
- PMCID: PMC7958270
- DOI: 10.2991/jegh.k.200823.001
Epidemic Landscape and Forecasting of SARS-CoV-2 in India
Abstract
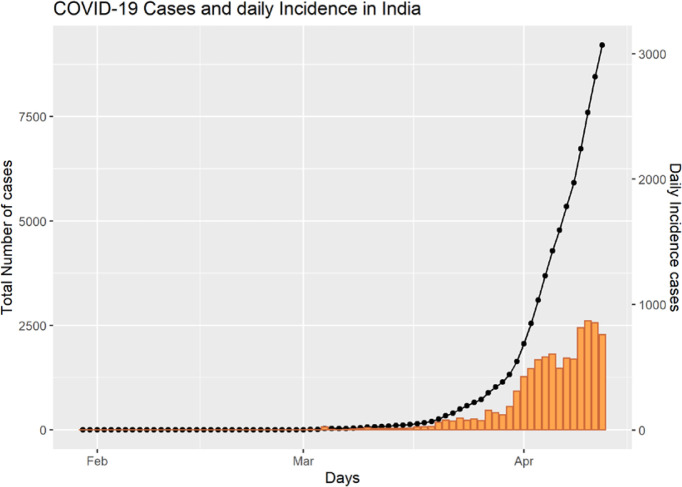
Background: India was one of the countries to institute strict measures for Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) control in the early phase. Since, then, the epidemic growth trajectory was slow before registering an explosion of cases due to local cluster transmissions.
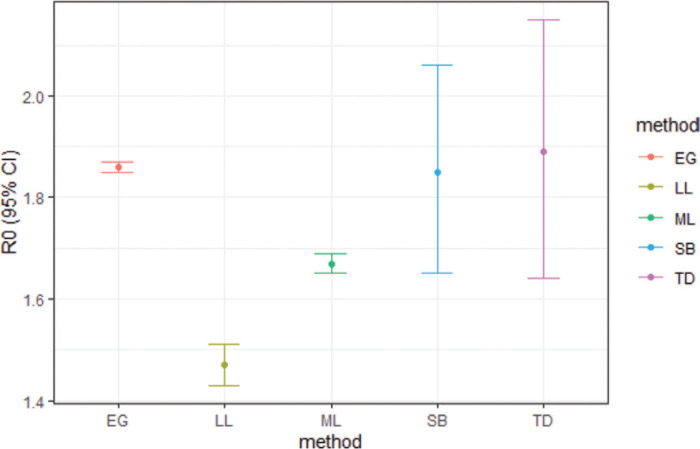
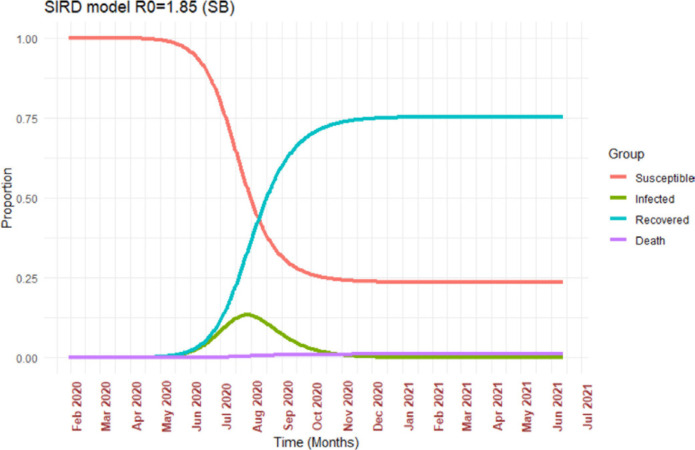
Methods: We estimated the growth rate and doubling time of SARS-CoV-2 for India and high burden states using crowdsourced time series data. Further, we also estimated the Basic Reproductive Number (R0) and Time-dependent Reproductive number (Rt) using serial intervals from the data. We compared the R0 estimated from five different methods and R0 from SB was further used in the analysis. We modified standard Susceptible-Infectious-Recovered (SIR) models to SIR/Death (SIRD) model to accommodate deaths using R0 with the sequential Bayesian method for simulation in SIRD models.
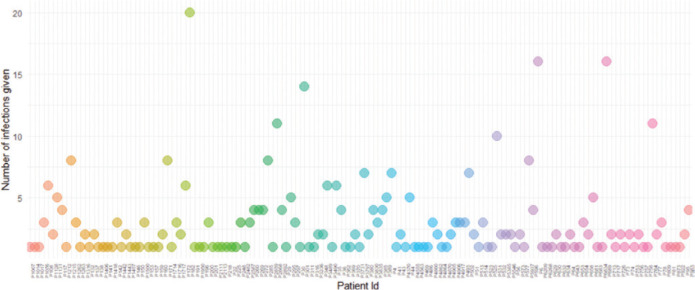
Results: On average, 2.8 individuals were infected by an index case. The mean serial interval was 3.9 days. The R0 estimated from different methods ranged from 1.43 to 1.85. The mean time to recovery was 14 ± 5.3 days. The daily epidemic growth rate of India was 0.16 [95% CI; 0.14, 0.17] with a doubling time of 4.30 days [95% CI; 3.96, 4.70]. From the SIRD model, it can be deduced that the peak of SARS-CoV-2 in India will be around mid-July to early August 2020 with around 12.5% of the population likely to be infected at the peak time.
Conclusion: The pattern of spread of SARS-CoV-2 in India is suggestive of community transmission. There is a need to increase funds for infectious disease research and epidemiologic studies. All the current gains may be reversed if air travel and social mixing resume rapidly. For the time being, these must be resumed only in a phased manner and should be back to normal levels only after we are prepared to deal with the disease with efficient tools like vaccines or medicine.
Question: What are the estimates of infectious disease parameters of early phase of novel SARS-CoV-2 epidemic in India?
Findings: Incidence pattern SARS-CoV-2 shows possible evidence of community transmission. However, the estimated Basic Reproductive Number (R0) is relatively lower than those observed in high burden regions (range 1.43-1.85). Our simulation using susceptible-infectious-recovered/death model shows that peak of SARS-CoV-2 in India is farther than currently projected and is likely to affect around 12.5% of population.
Meaning: The lower estimated R0 is indicative of the effectiveness of early social distancing measures and lockdown. Premature relaxation of the current control measures may result in large numbers of cases in India.
Keywords: COVID-19; India; R0; Rt.
© 2020 The Authors. Published by Atlantis Press International B.V.
Conflict of interest statement
The authors declare they have no conflicts of interest.
Figures
References
-
- Worldometer . Worldometer; 2020. Coronavirus cases [Internet] pp. 1–22. Available from: https://www.worldometers.info/coronavirus/coronavirus-cases/#daily-cases [cited April 10, 2020].
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous