

Association of Medicare Mandatory Bundled Payment System for Hip and Knee Joint Replacement With Racial/Ethnic Difference in Joint Replacement Care
- PMID: 32960277
- PMCID: PMC7509636
- DOI: 10.1001/jamanetworkopen.2020.14475
Association of Medicare Mandatory Bundled Payment System for Hip and Knee Joint Replacement With Racial/Ethnic Difference in Joint Replacement Care
Abstract
Importance: There are marked racial/ethnic differences in hip and knee joint replacement care as well as concerns that value-based payments may exacerbate existing racial/ethnic disparities in care.
Objective: To examine changes in joint replacement care associated with Medicare's Comprehensive Care for Joint Replacement (CJR) model among White, Black, and Hispanic patients.
Design, setting, and participants: Retrospective cohort study of Medicare claims from 2013 through 2017 among White, Black, and Hispanic patients undergoing joint replacement in 67 treatment (selected for CJR participation) and 103 control metropolitan statistical areas.
Exposures: The CJR model holds hospitals accountable for spending and quality of joint replacement care during care episodes (index hospitalization through 90 days after discharge).
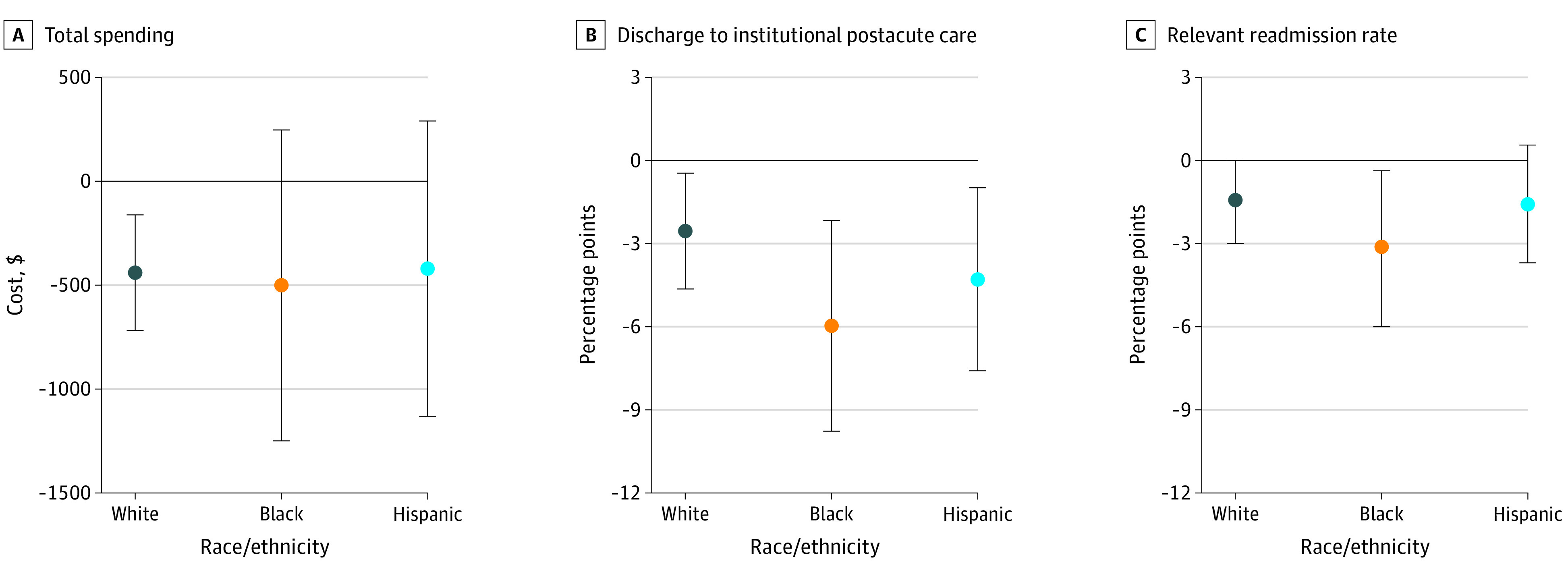
Main outcomes and measures: The primary outcomes were spending, discharge to institutional postacute care, and readmission during care episodes.
Results: Among 688 346 patients, 442 163 (64.2%) were women, and 87 286 (12.7%) were 85 years or older. Under CJR, spending decreased by $439 for White patients (95% CI, -$718 to -$161; from pre-CJR spending in treatment metropolitan statistical areas of $25 264) but did not change for Black patients and Hispanic patients. Discharges to institutional postacute care decreased for all groups (-2.5 percentage points; 95% CI, -4.7 to -0.4, from pre-CJR risk of 46.2% for White patients; -6.0 percentage points; 95% CI, -9.8 to -2.2, from pre-CJR risk of 59.5% for Black patients; and -4.3 percentage points; 95% CI, -7.6 to -1.0, from pre-CJR risk of 54.3% for Hispanic patients). Readmission risk decreased for Black patients by 3.1 percentage points (95% CI, -5.9 to -0.4, from pre-CJR risk of 21.8%) and did not change for White patients and Hispanic patients. Under CJR, Black-White differences in discharges to institutional postacute care decreased by 3.4 percentage points (95% CI, -6.4 to -0.5, from the pre-CJR Black-White difference of 13.3 percentage points). No evidence was found demonstrating that Black-White differences changed for other outcomes or that Hispanic-White differences changed for any outcomes under CJR.
Conclusions and relevance: In this cohort study of patients receiving joint replacements, CJR was associated with decreased readmissions for Black patients. Furthermore, Black patients experienced a greater decrease in discharges to institutional postacute care relative to White patients, representing relative improvements despite concerns that value-based payment models may exacerbate existing disparities. Nonetheless, differences between White and Black patients in joint replacement care still persisted even after these changes.
Conflict of interest statement
Figures
Similar articles
-
Association of Medicare Mandatory Bundled Payment Program With the Receipt of Elective Hip and Knee Replacement in White, Black, and Hispanic Beneficiaries.JAMA Netw Open. 2021 Mar 1;4(3):e211772. doi: 10.1001/jamanetworkopen.2021.1772. JAMA Netw Open. 2021. PMID: 33749766 Free PMC article.
-
Association of the Comprehensive Care for Joint Replacement Model With Disparities in the Use of Total Hip and Total Knee Replacement.JAMA Netw Open. 2021 May 3;4(5):e2111858. doi: 10.1001/jamanetworkopen.2021.11858. JAMA Netw Open. 2021. PMID: 34047790 Free PMC article.
-
Mandatory Medicare Bundled Payment Program for Lower Extremity Joint Replacement and Discharge to Institutional Postacute Care: Interim Analysis of the First Year of a 5-Year Randomized Trial.JAMA. 2018 Sep 4;320(9):892-900. doi: 10.1001/jama.2018.12346. JAMA. 2018. PMID: 30193277 Free PMC article. Clinical Trial.
-
Lessons Learned From the Comprehensive Care for Joint Replacement Model at an Academic Tertiary Center: The Good, the Bad, and the Ugly.J Arthroplasty. 2023 Jul;38(7 Suppl 2):S54-S62. doi: 10.1016/j.arth.2023.02.014. Epub 2023 Feb 11. J Arthroplasty. 2023. PMID: 36781061 Free PMC article. Review.
-
Relative-Value Units in Arthroplasty: Past, Present, and Future.J Arthroplasty. 2025 Feb;40(2):280-283. doi: 10.1016/j.arth.2024.11.032. Epub 2024 Nov 22. J Arthroplasty. 2025. PMID: 39579803 Review.
Cited by
-
The Spillover Effect of the Medicare Mandatory Bundled Payment Program on Joint Replacement Outcomes: Analysis of Patients with Commercial Insurance and Medicare Advantage.J Bone Joint Surg Am. 2022 Apr 6;104(7):621-629. doi: 10.2106/JBJS.21.00259. Epub 2021 Dec 13. J Bone Joint Surg Am. 2022. PMID: 34898513 Free PMC article.
-
Outcomes by Race and Ethnicity Following a Medicare Bundled Payment Program for Joint Replacement.JAMA Netw Open. 2024 Sep 3;7(9):e2433962. doi: 10.1001/jamanetworkopen.2024.33962. JAMA Netw Open. 2024. PMID: 39287943 Free PMC article.
-
Two Decades Since the Unequal Treatment Report: The State of Racial, Ethnic, and Socioeconomic Disparities in Elective Total Hip and Knee Replacement Use.J Bone Joint Surg Am. 2025 Mar 5;107(5):523-538. doi: 10.2106/JBJS.24.00347. Epub 2024 Nov 20. J Bone Joint Surg Am. 2025. PMID: 39813469 Review.
-
Association of Medicare Mandatory Bundled Payment Program With the Receipt of Elective Hip and Knee Replacement in White, Black, and Hispanic Beneficiaries.JAMA Netw Open. 2021 Mar 1;4(3):e211772. doi: 10.1001/jamanetworkopen.2021.1772. JAMA Netw Open. 2021. PMID: 33749766 Free PMC article.
-
Medicare's comprehensive care for joint replacement model increased public hospitals' inpatient length of stay.BMC Health Serv Res. 2024 Nov 28;24(1):1495. doi: 10.1186/s12913-024-11905-0. BMC Health Serv Res. 2024. PMID: 39609805 Free PMC article.
References
-
- Center for Medicare & Medicaid Services Comprehensive Care for Joint Replacement (CJR) Model. Center for Medicare & Medicaid Services ; 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
