

Effects of mavacamten on Ca2+ sensitivity of contraction as sarcomere length varied in human myocardium
- PMID: 32960449
- PMCID: PMC7707091
- DOI: 10.1111/bph.15271
Effects of mavacamten on Ca2+ sensitivity of contraction as sarcomere length varied in human myocardium
Abstract
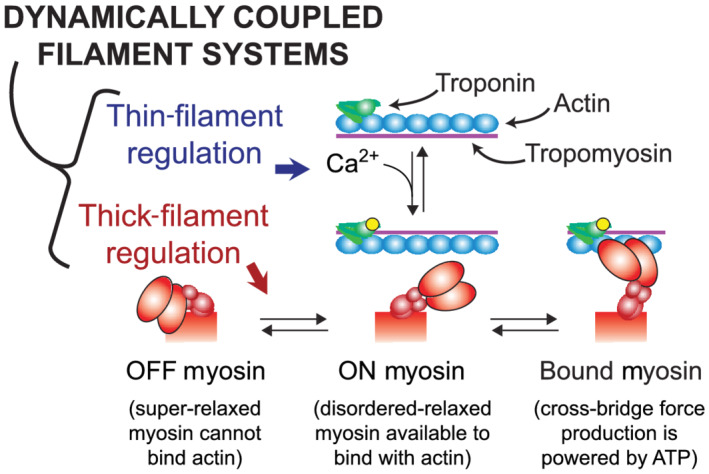
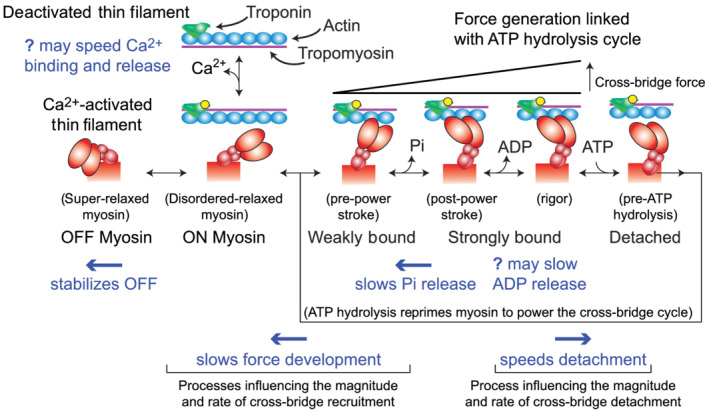
Background and purpose: Heart failure can reflect impaired contractile function at the myofilament level. In healthy hearts, myofilaments become more sensitive to Ca2+ as cells are stretched. This represents a fundamental property of the myocardium that contributes to the Frank-Starling response, although the molecular mechanisms underlying the effect remain unclear. Mavacamten, which binds to myosin, is under investigation as a potential therapy for heart disease. We investigated how mavacamten affects the sarcomere-length dependence of Ca2+ -sensitive isometric contraction to determine how mavacamten might modulate the Frank-Starling mechanism.
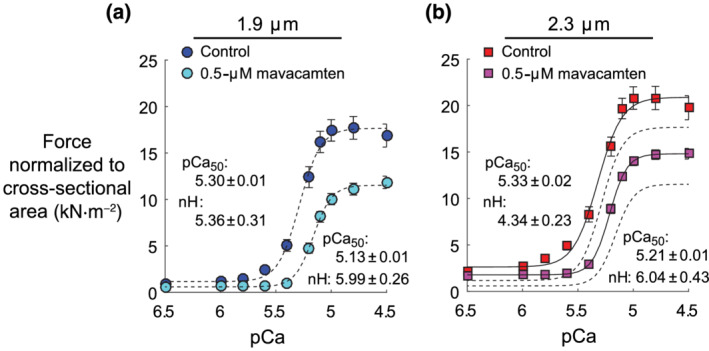
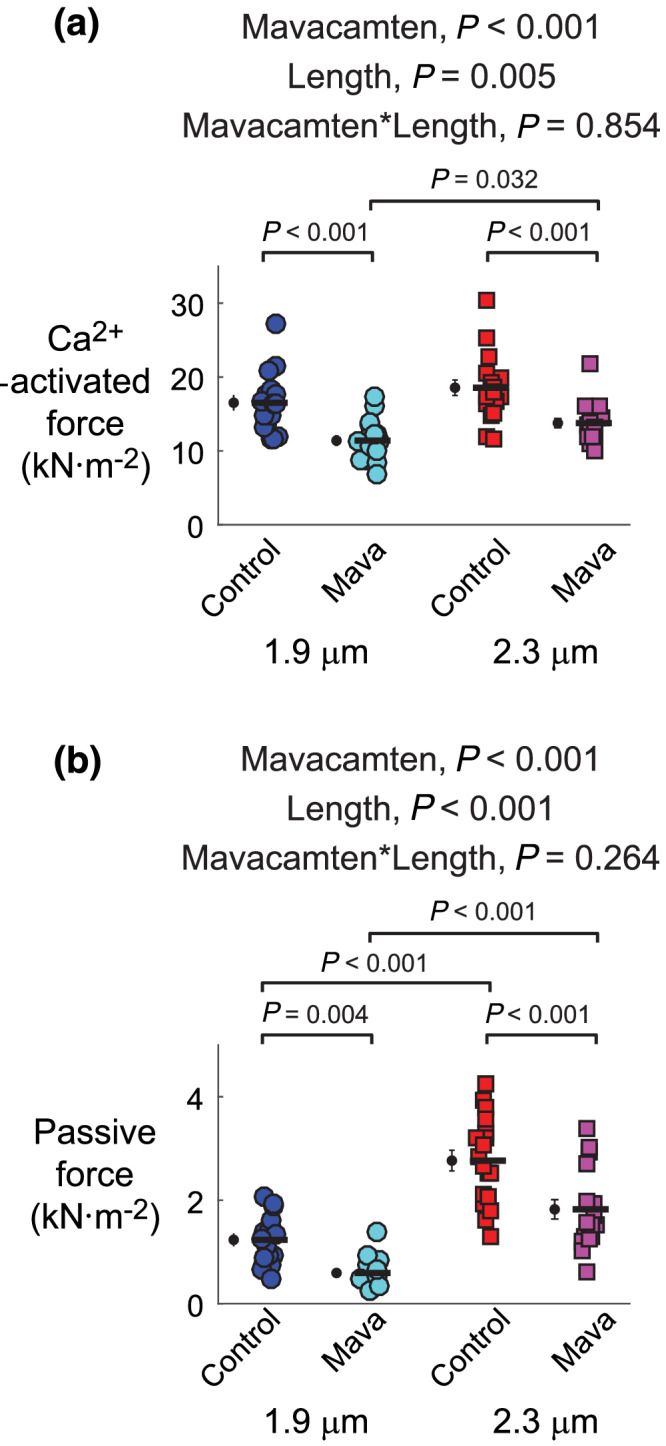
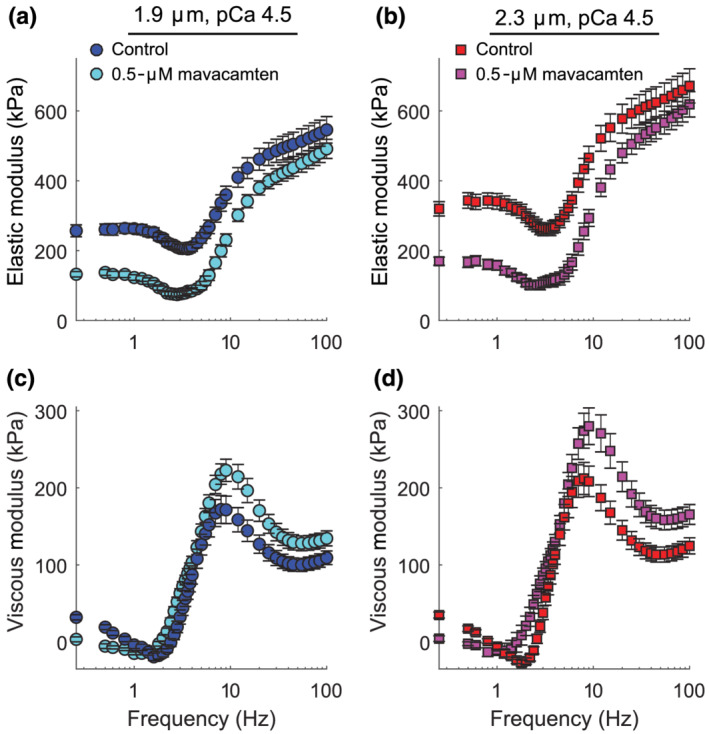
Experimental approach: Multicellular preparations from the left ventricular-free wall of hearts from organ donors were chemically permeabilized and Ca2+ activated in the presence or absence of 0.5-μM mavacamten at 1.9 or 2.3-μm sarcomere length (37°C). Isometric force and frequency-dependent viscoelastic myocardial stiffness measurements were made.
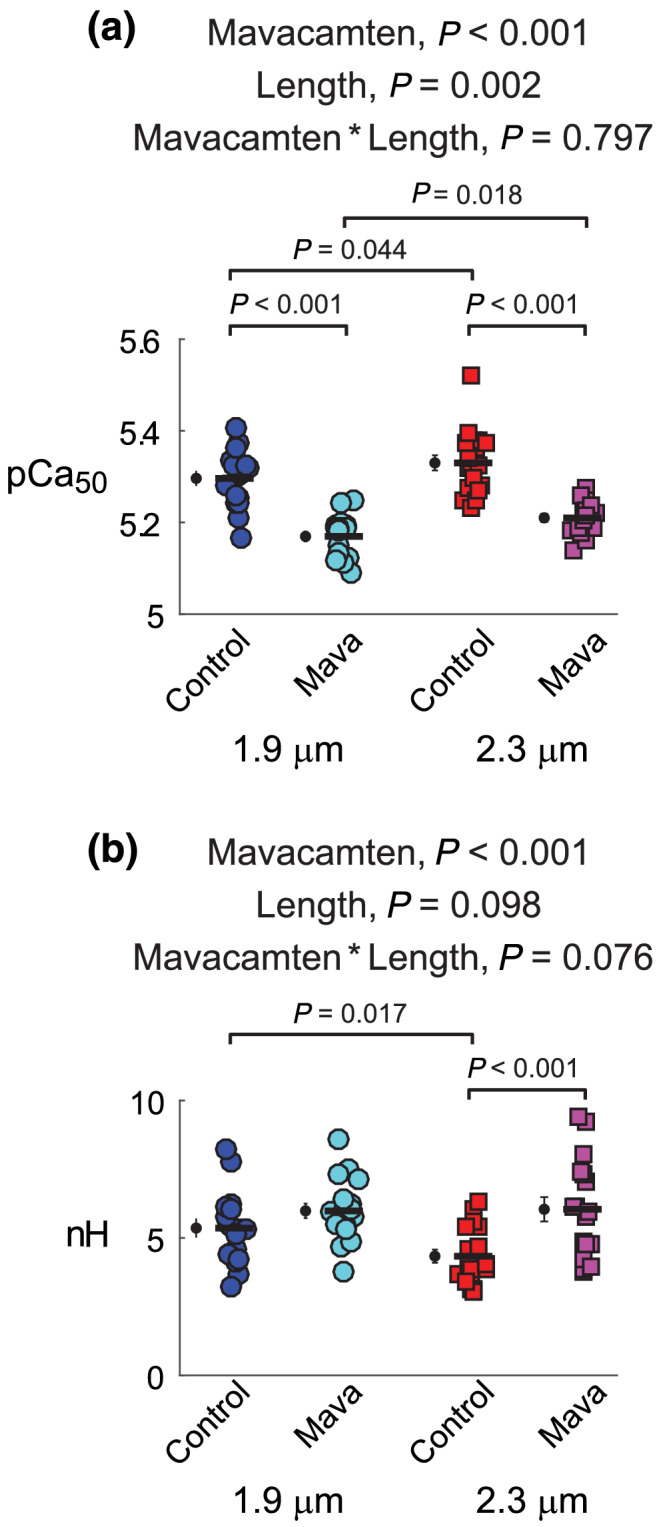
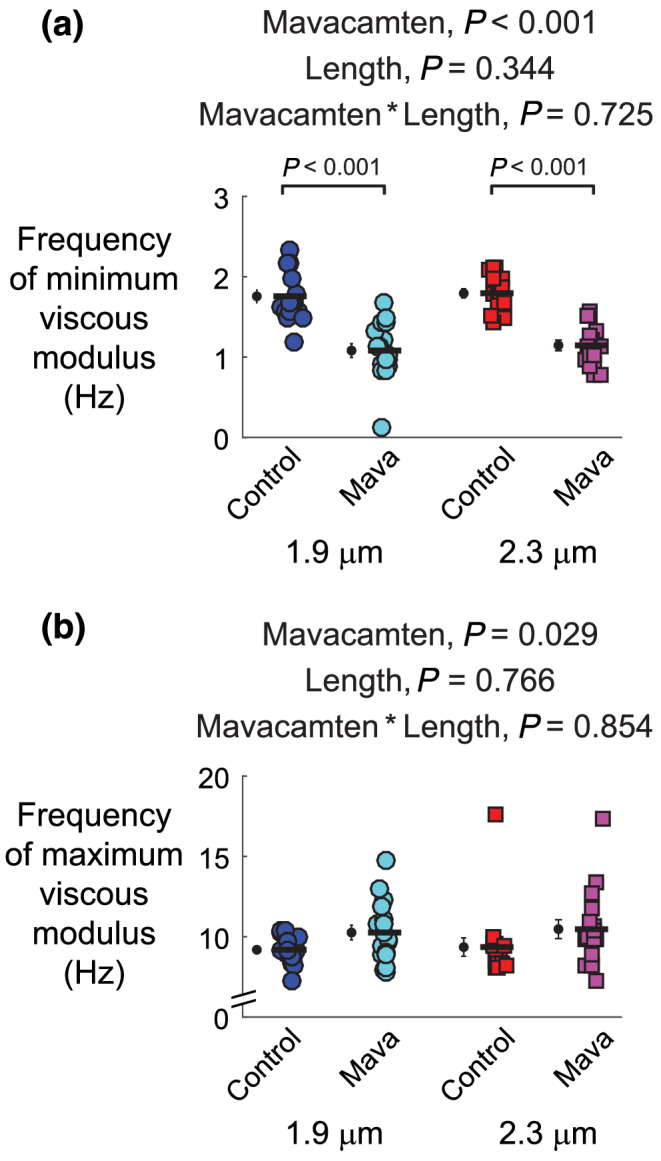
Key results: At both sarcomere lengths, mavacamten reduced maximal force and Ca2+ sensitivity of contraction. In the presence and absence of mavacamten, Ca2+ sensitivity of force increased as sarcomere length increased. This suggests that the length-dependent activation response was maintained in human myocardium, even though mavacamten reduced Ca2+ sensitivity. There were subtle effects of mavacamten reducing force values under relaxed conditions (pCa 8.0), as well as slowing myosin cross-bridge recruitment and speeding cross-bridge detachment under maximally activated conditions (pCa 4.5).
Conclusion and implications: Mavacamten did not eliminate sarcomere length-dependent increases in the Ca2+ sensitivity of contraction in myocardial strips from organ donors at physiological temperature. Drugs that modulate myofilament function may be useful therapies for cardiomyopathies.
Keywords: cardiac muscle mechanics; human myosin; mavacamten; sarcomere length.
© 2020 The British Pharmacological Society.
Conflict of interest statement
The authors declare no competing financial interests and have nothing to disclose.
Figures
References
-
- Ait‐Mou, Y. , Hsu, K. , Farman, G. P. , Kumar, M. , Greaser, M. L. , Irving, T. C. , & de Tombe, P. P. (2016). Titin strain contributes to the Frank‐Starling law of the heart by structural rearrangements of both thin‐ and thick‐filament proteins. Proceedings of the National Academy of Sciences of the United States of America, 113, 2306–2311. 10.1073/pnas.1516732113 - DOI - PMC - PubMed
-
- Ambrosy, A. P. , Fonarow, G. C. , Butler, J. , Chioncel, O. , Greene, S. J. , Vaduganathan, M. , … Gheorghiade, M. (2014). The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. Journal of the American College of Cardiology, 63, 1123–1133. 10.1016/j.jacc.2013.11.053 - DOI - PubMed
-
- Anderson, R. L. , Trivedi, D. V. , Sarkar, S. S. , Henze, M. , Ma, W. , Gong, H. , … Spudich, J. A. (2018). Deciphering the super relaxed state of human beta‐cardiac myosin and the mode of action of mavacamten from myosin molecules to muscle fibers. Proceedings of the National Academy of Sciences of the United States of America, 115, E8143–E8152. 10.1073/pnas.1809540115 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
