

Enhanced treatment strategies and distinct disease outcomes among autoantibody-positive and -negative rheumatoid arthritis patients over 25 years: A longitudinal cohort study in the Netherlands
- PMID: 32960885
- PMCID: PMC7508377
- DOI: 10.1371/journal.pmed.1003296
Enhanced treatment strategies and distinct disease outcomes among autoantibody-positive and -negative rheumatoid arthritis patients over 25 years: A longitudinal cohort study in the Netherlands
Abstract
Background: Based on different genetic and environmental risk factors and histology, it has been proposed that rheumatoid arthritis (RA) consists of 2 types: autoantibody-positive and autoantibody-negative RA. However, until now, this remained hypothetical. To assess this hypothesis, we studied whether the long-term outcomes differed for these 2 groups of RA patients.
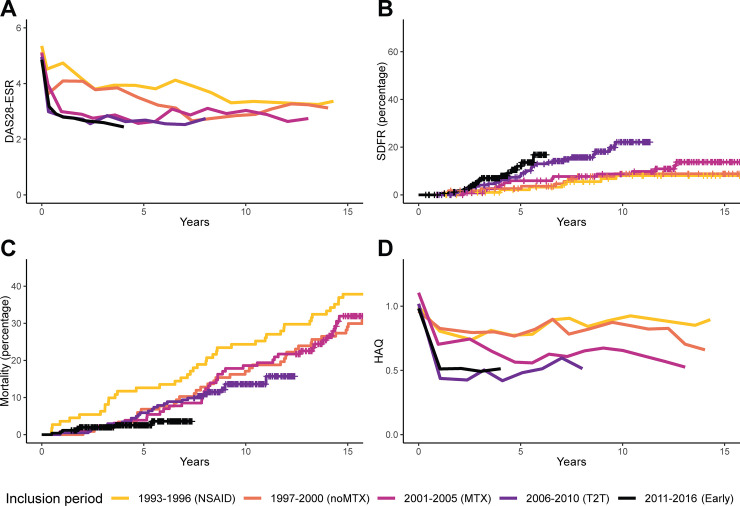
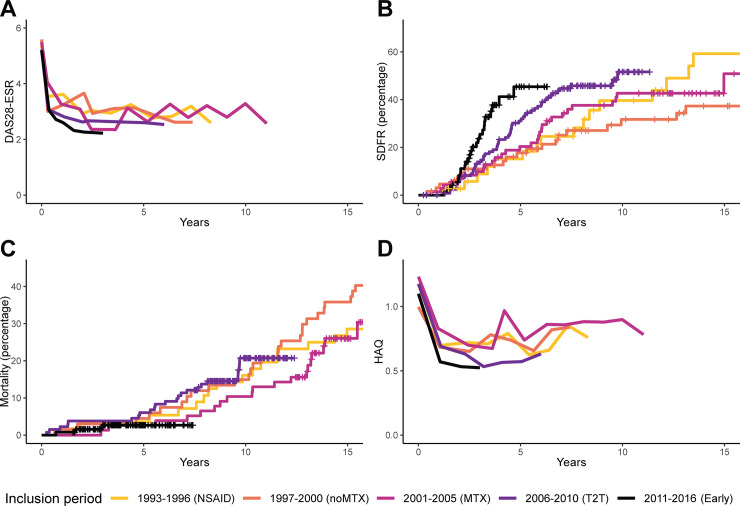
Methods and findings: In the Leiden Early Arthritis Clinic cohort, 1,285 consecutive RA patients were included between 1993 and 2016 and followed yearly. Treatment protocols in routine care improved over time, irrespective of autoantibody status, and 5 inclusion periods were used as instrumental variables: 1993-1996, delayed mild disease-modifying antirheumatic drug (DMARD) initiation (reference period); 1997-2000, early mild DMARDs; 2001-2005, early methotrexate; 2006-2010, early methotrexate followed by treat-to-target adjustments; 2011-2016, similar to 2006-2010 plus additional efforts for very early referral. Three long-term outcomes were studied: sustained DMARD-free remission (SDFR) (persistent absence of clinical synovitis after DMARD cessation), mortality, and functional disability measured by yearly Health Assessment Questionnaire (HAQ). Treatment response in the short term (disease activity) was measured by Disease Activity Score-28 with erythrocyte sedimentation rate (DAS28-ESR). Linear mixed models and Cox regression were used, stratified for autoantibody positivity, defined as IgG anti-CCP2 and/or IgM rheumatoid factor positivity. In total, 823 patients had autoantibody-positive RA (mean age 55 years, 67% female); 462 patients had autoantibody-negative RA (age 60 years, 64% female). Age, gender, and percentage of autoantibody-positive patients were stable throughout the inclusion periods. Disease activity significantly decreased over time within both groups. SDFR rates increased after introduction of treat-to-target (hazard ratio [HR] 2006-2010 relative to 1993-1996: 3.35 [95% CI 1.46 to 7.72; p = 0.004]; HR 2011-2016: 4.57 [95% CI 1.80 to 11.6; p = 0.001]) in autoantibody-positive RA, but not in autoantibody-negative RA. In autoantibody-positive RA, mortality decreased significantly after the introduction of treat-to-target treatment adjustments (HR 2006-2010: 0.56 [95% CI 0.34 to 0.92; p = 0.023]; HR 2011-2016: 0.33 [95% CI 0.14 to 0.77; p = 0.010]), but not in autoantibody-negative RA (HR 2006-2010: 0.79 [95% CI 0.40 to 1.56; p = 0.50]; HR 2011-2016: 0.36 [95% CI 0.10 to 1.34; p = 0.13]). Similarly, functional disability improved in autoantibody-positive RA for the periods after 2000 relative to 1993-1996 (range -0.16 [95% CI -0.29 to -0.03; p = 0.043] to -0.32 [95% CI -0.44 to -0.20; p < 0.001] units of improvement), but not in autoantibody-negative RA (range 0.10 [95% CI -0.12 to 0.31; p = 0.38] to -0.13 [95% CI -0.34 to 0.07; p = 0.20] units of improvement). Limitations to note were that treatment was not randomized-but it was protocolized and instrumental variable analysis was used to obtain comparable groups-and that a limited spread of ethnicities was included.
Conclusions: Although disease activity has improved in both autoantibody-positive and autoantibody-negative RA in recent decades, the response in long-term outcomes differed. We propose that it is time to subdivide RA into autoantibody-positive RA (type 1) and autoantibody-negative RA (type 2), in the hope that this leads to stratified treatment in RA.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: TH is a member of the Editorial Board of PLOS Medicine.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
