

Cytokine storm and COVID-19: a chronicle of pro-inflammatory cytokines
- PMID: 32961074
- PMCID: PMC7536084
- DOI: 10.1098/rsob.200160
Cytokine storm and COVID-19: a chronicle of pro-inflammatory cytokines
Abstract
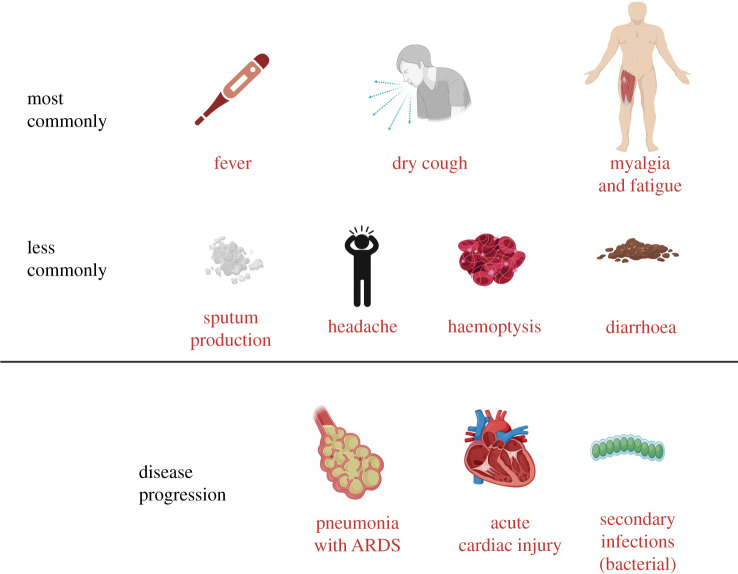
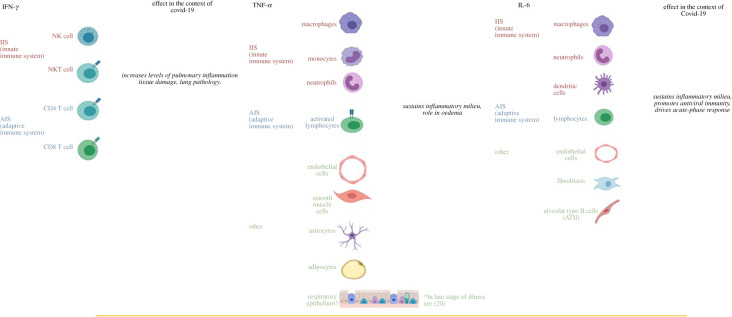
Coronavirus disease 2019 (COVID-19) has swept the world, unlike any other pandemic in the last 50 years. Our understanding of the disease has evolved rapidly since the outbreak; disease prognosis is influenced mainly by multi-organ involvement. Acute respiratory distress syndrome, heart failure, renal failure, liver damage, shock and multi-organ failure are strongly associated with morbidity and mortality. The COVID-19 disease pathology is plausibly linked to the hyperinflammatory response of the body characterized by pathological cytokine levels. The term 'cytokine storm syndrome' is perhaps one of the critical hallmarks of COVID-19 disease severity. In this review, we highlight prominent cytokine families and their potential role in COVID-19, the type I and II interferons, tumour necrosis factor and members of the Interleukin family. We address various changes in cellular components of the immune response corroborating with changes in cytokine levels while discussing cytokine sources and biological functions. Finally, we discuss in brief potential therapies attempting to modulate the cytokine storm.
Keywords: COVID-19; IFN-γ; IL-6; SARS; TNF-α; coronavirus.
Conflict of interest statement
We declare we have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous