

Characteristics and Outcomes of Individuals With Pre-existing Kidney Disease and COVID-19 Admitted to Intensive Care Units in the United States
- PMID: 32961244
- PMCID: PMC7501875
- DOI: 10.1053/j.ajkd.2020.09.003
Characteristics and Outcomes of Individuals With Pre-existing Kidney Disease and COVID-19 Admitted to Intensive Care Units in the United States
Abstract
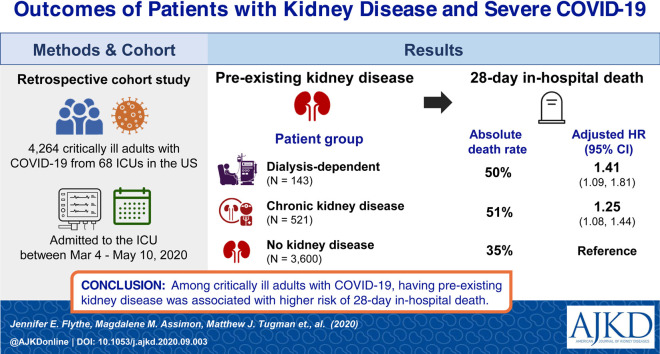
Rationale & objective: Underlying kidney disease is an emerging risk factor for more severe coronavirus disease 2019 (COVID-19) illness. We examined the clinical courses of critically ill COVID-19 patients with and without pre-existing chronic kidney disease (CKD) and investigated the association between the degree of underlying kidney disease and in-hospital outcomes.
Study design: Retrospective cohort study.
Settings & participants: 4,264 critically ill patients with COVID-19 (143 patients with pre-existing kidney failure receiving maintenance dialysis; 521 patients with pre-existing non-dialysis-dependent CKD; and 3,600 patients without pre-existing CKD) admitted to intensive care units (ICUs) at 68 hospitals across the United States.
Predictor(s): Presence (vs absence) of pre-existing kidney disease.
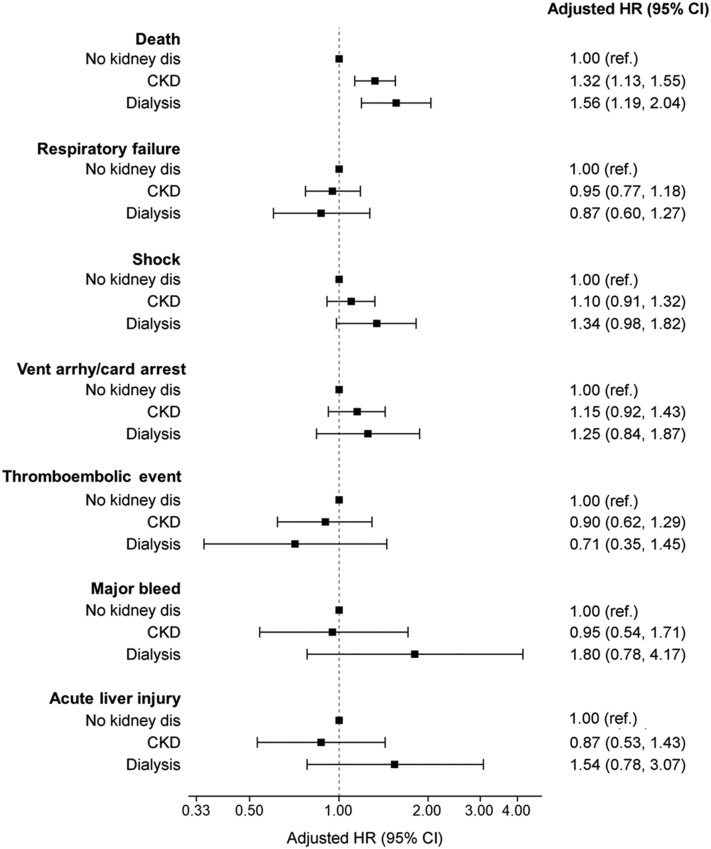
Outcome(s): In-hospital mortality (primary); respiratory failure, shock, ventricular arrhythmia/cardiac arrest, thromboembolic events, major bleeds, and acute liver injury (secondary).
Analytical approach: We used standardized differences to compare patient characteristics (values>0.10 indicate a meaningful difference between groups) and multivariable-adjusted Fine and Gray survival models to examine outcome associations.
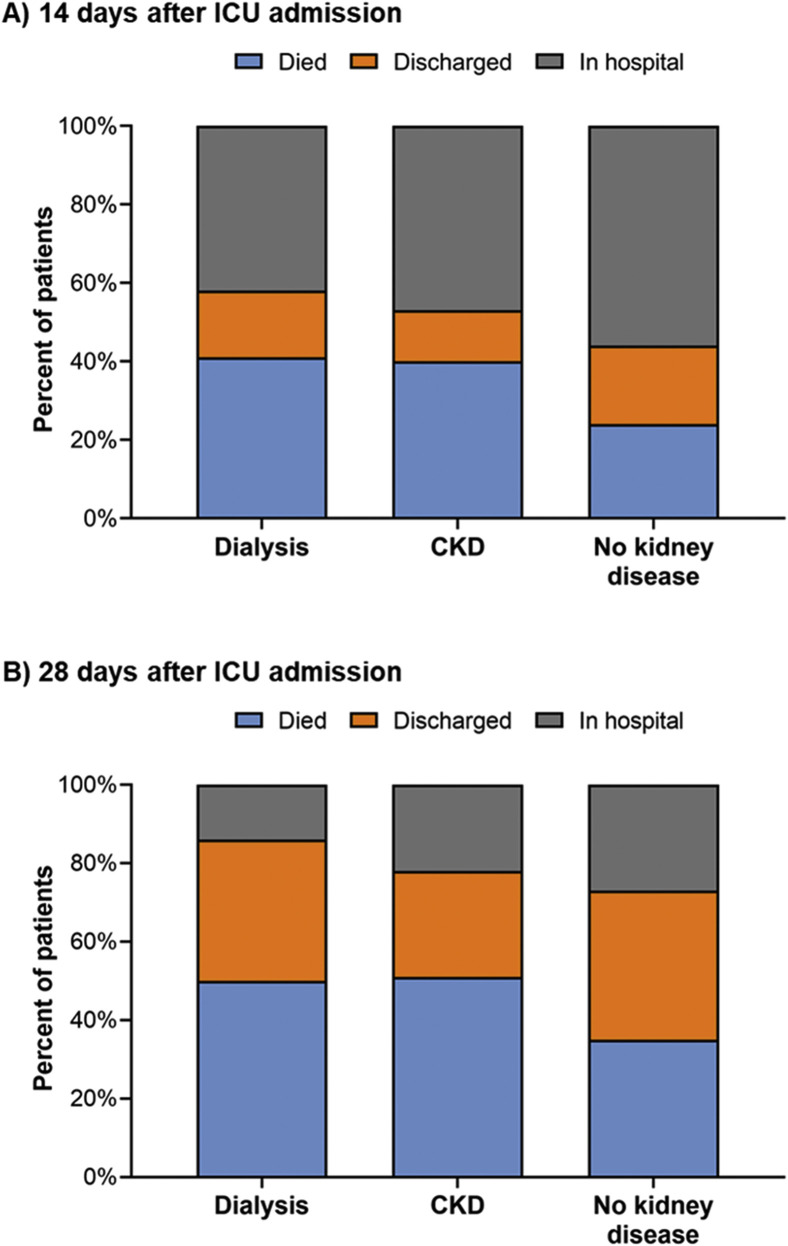
Results: Dialysis patients had a shorter time from symptom onset to ICU admission compared to other groups (median of 4 [IQR, 2-9] days for maintenance dialysis patients; 7 [IQR, 3-10] days for non-dialysis-dependent CKD patients; and 7 [IQR, 4-10] days for patients without pre-existing CKD). More dialysis patients (25%) reported altered mental status than those with non-dialysis-dependent CKD (20%; standardized difference=0.12) and those without pre-existing CKD (12%; standardized difference=0.36). Half of dialysis and non-dialysis-dependent CKD patients died within 28 days of ICU admission versus 35% of patients without pre-existing CKD. Compared to patients without pre-existing CKD, dialysis patients had higher risk for 28-day in-hospital death (adjusted HR, 1.41 [95% CI, 1.09-1.81]), while patients with non-dialysis-dependent CKD had an intermediate risk (adjusted HR, 1.25 [95% CI, 1.08-1.44]).
Limitations: Potential residual confounding.
Conclusions: Findings highlight the high mortality of individuals with underlying kidney disease and severe COVID-19, underscoring the importance of identifying safe and effective COVID-19 therapies in this vulnerable population.
Keywords: COVID-19 outcome; Coronavirus disease 2019 (COVID-19); altered mental status; chronic kidney disease (CKD); clinical course; clinical trajectory; critical illness; dialysis; end-stage kidney disease (ESKD); end-stage renal disease (ESRD); glomerular filtration rate (GFR); in-hospital mortality; intensive care unit (ICU); prognosis; renal function; severe COVID-19; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Copyright © 2020 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
COVID-19: The Kidneys Tell a Tale.Am J Kidney Dis. 2021 Feb;77(2):175-177. doi: 10.1053/j.ajkd.2020.11.001. Epub 2020 Dec 17. Am J Kidney Dis. 2021. PMID: 33342610 Free PMC article. No abstract available.
-
Combination therapy for COVID-19 in hemodialysis patients: Pharmacological treatments and renal replacement therapy based on the severity.Ther Apher Dial. 2022 Apr;26(2):475-477. doi: 10.1111/1744-9987.13737. Epub 2021 Sep 22. Ther Apher Dial. 2022. PMID: 34533292 Free PMC article. No abstract available.
References
-
- Johns Hopkins University Coronavirus Resource Center, 2020. https://coronavirus.jhu.edu/ Accessed September 13, 2020.
Publication types
MeSH terms
Grants and funding
- K23 HL143053/HL/NHLBI NIH HHS/United States
- R01 DK125786/DK/NIDDK NIH HHS/United States
- P30 DK079310/DK/NIDDK NIH HHS/United States
- R01 DK113191/DK/NIDDK NIH HHS/United States
- K23 DK109401/DK/NIDDK NIH HHS/United States
- R01 HL153384/HL/NHLBI NIH HHS/United States
- K23 DK101826/DK/NIDDK NIH HHS/United States
- K23 HL130648/HL/NHLBI NIH HHS/United States
- R01 HL144566/HL/NHLBI NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- K23 DK116967/DK/NIDDK NIH HHS/United States
- R01 HL152034/HL/NHLBI NIH HHS/United States
- K23 DK120811/DK/NIDDK NIH HHS/United States
- UL1 TR002389/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
