

Combining Correlated Outcomes and Surrogate Endpoints in a Network Meta-Analysis of Colorectal Cancer Treatments
- PMID: 32961943
- PMCID: PMC7565292
- DOI: 10.3390/cancers12092663
Combining Correlated Outcomes and Surrogate Endpoints in a Network Meta-Analysis of Colorectal Cancer Treatments
Abstract
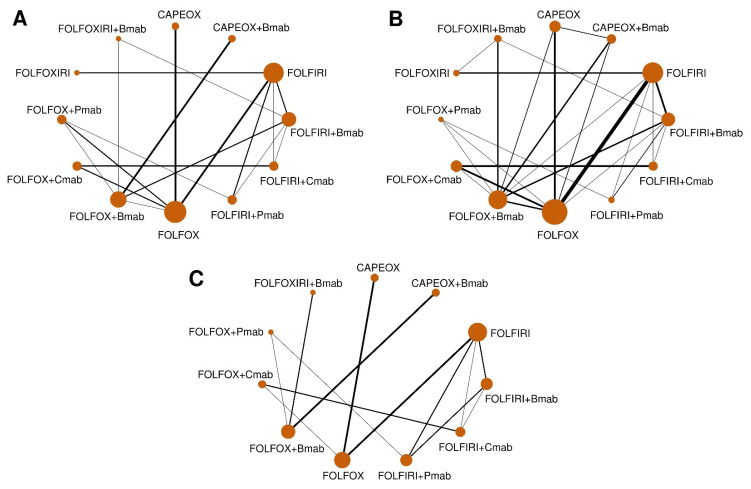
This study aimed to investigate the efficacy and safety of systemic therapies in the treatment of unresectable advanced or metastatic colorectal cancer. Predicted hazard ratios (HRs) and their 95% credible intervals (CrIs) for overall survival (OS) were calculated from the odds ratio (OR) for the overall response rate and/or HR for progression-free survival using multivariate random effects (MVRE) models. We performed a network meta-analysis (NMA) of 49 articles to compare the efficacy and safety of FOLFOX/FOLFIRI±bevacizumab (Bmab)/cetuximab (Cmab)/panitumumab (Pmab), and FOLFOXIRI/CAPEOX±Bmab. The NMA showed significant OS improvement with FOLFOX, FOLFOX+Cmab, and FOLFIRI+Cmab compared with that of FOLFIRI (HR = 0.84, 95% CrI = 0.73-0.98; HR = 0.76, 95% CrI = 0.62-0.94; HR = 0.80, 95% CrI = 0.66-0.96, respectively), as well as with FOLFOX+Cmab and FOLFIRI+Cmab compared with that of FOLFOXIRI (HR = 0.69, 95% CrI = 0.51-0.94 and HR = 0.73, 95% CrI = 0.54-0.97, respectively). The odds of adverse events grade ≥3 were significantly higher for FOLFOX+Cmab vs. FOLFIRI+Bmab (OR = 2.34, 95% CrI = 1.01-4.66). Higher odds of events were observed for FOLFIRI+Pmab in comparison with FOLFIRI (OR = 2.16, 95% CrI = 1.09-3.84) and FOLFIRI+Bmab (OR = 3.14, 95% CrI = 1.51-5.89). FOLFOX+Cmab and FOLFIRI+Bmab showed high probabilities of being first- and second-line treatments in terms of the efficacy and safety, respectively. The findings of the efficacy and safety comparisons may support the selection of appropriate treatments in clinical practice. PROSPERO registration: CRD42020153640.
Keywords: colorectal cancer; network meta-analysis; surrogate endpoints.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- National Comprehensive Cancer Network (NCCN) Guidelines for Patients. Colon Cancer. [(accessed on 4 July 2019)]; Available online: https://www.nccn.org/patients/guidelines/colon/files/assets/common/downl....
-
- National Comprehensive Cancer Network (NCCN) Guidelines for Patients. Rectal Cancer. [(accessed on 4 July 2019)]; Available online: https://www.nccn.org/patients/guidelines/rectal/files/assets/common/down....
Grants and funding
LinkOut - more resources
Full Text Sources
