

Endoscopic Ultrasonography-Guided Gastroenterostomy Techniques for Treatment of Malignant Gastric Outlet Obstruction
- PMID: 32962331
- PMCID: PMC7548149
- DOI: 10.5946/ce.2020.151
Endoscopic Ultrasonography-Guided Gastroenterostomy Techniques for Treatment of Malignant Gastric Outlet Obstruction
Abstract
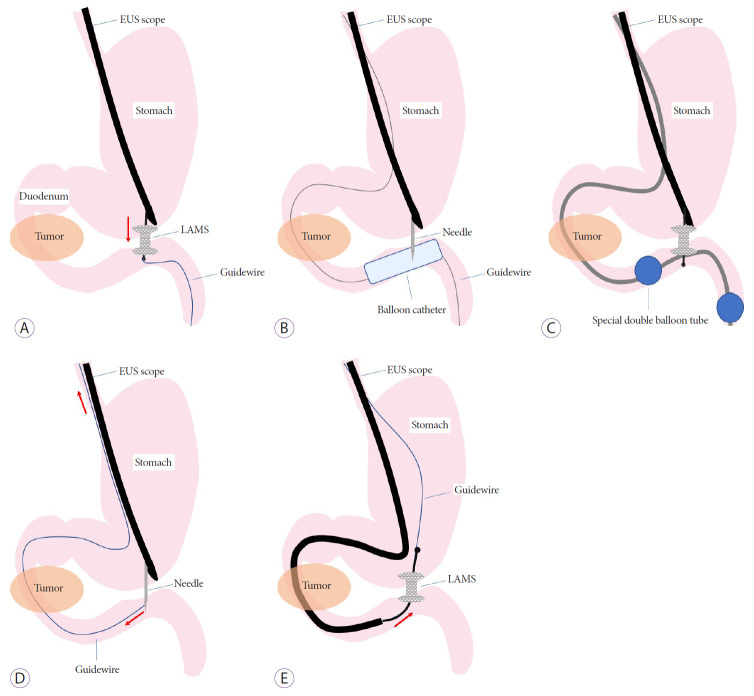
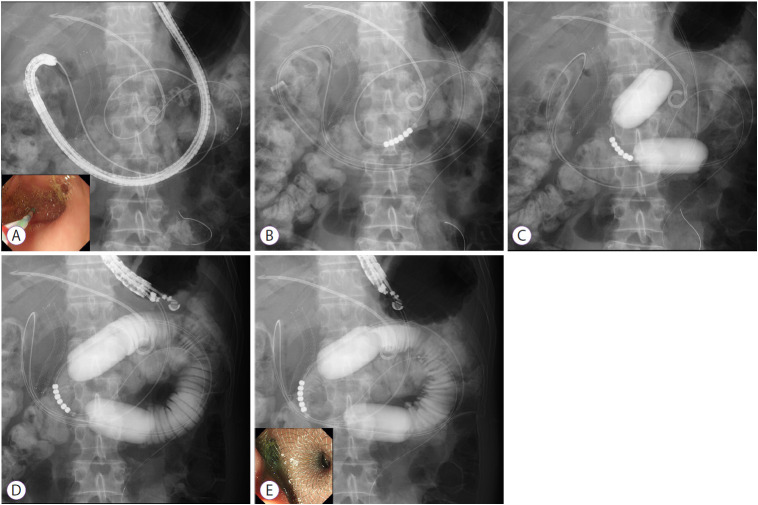
Gastric outlet obstruction (GOO) can be caused by periampullary malignancies and often leads to a reduction in a patient's quality of life. Recently, endoscopic ultrasonography-guided gastroenterostomy (EUS-GE) using a lumen-apposing self-expandable metal stent (LAMS) has been developed as a minimally invasive and durable endoscopic treatment for GOO. There are three types of EUS-GE technique: (1) the direct technique; (2) device-assisted techniques, such as a balloon catheter, nasobiliary drainage tube, and ultraslim endoscopy; and (3) EUS-guided double balloon-occluded gastrojejunostomy bypass. Previous reports of EUS-GE with LAMS have shown technical and clinical success rates (regardless of technique and etiology) of 87%-100% and 84%-100%, respectively. Studies comparing EUS-GE and surgical gastrojejunostomy have shown similar success rates, reintervention rates, and cost benefits, with a lower rate of early adverse events in EUS-GE. A comparison of EUS-GE and endoscopic enteral stent placement revealed similar technical success rates, but initial clinical success rate was higher and the rate of stent failure requiring reintervention was lower with EUS-GE.
Keywords: Duodenal obstruction; Endosonography; Gastric bypass; Gastric outlet obstruction; Gastroenterostomy.
Conflict of interest statement
Figures
References
-
- Tringali A, Didden P, Repici A, et al. Endoscopic treatment of malignant gastric and duodenal strictures: a prospective, multicenter study. Gastrointest Endosc. 2014;79:66–75. - PubMed
-
- Conio M, Demarquay JF, De Luca L, Marchi S, Dumas R. Endoscopic treatment of pancreatico-biliary malignancies. Crit Rev Oncol Hematol. 2001;37:127–135. - PubMed
-
- Tendler DA. Malignant gastric outlet obstruction: bridging another divide. Am J Gastroenterol. 2002;97:4–6. - PubMed
-
- Maetani I, Inoue H, Sato M, Ohashi S, Igarashi Y, Sakai Y. Peroral insertion techniques of self-expanding metal stents for malignant gastric outlet and duodenal stenoses. Gastrointest Endosc. 1996;44:468–471. - PubMed
-
- Khashab M, Alawad AS, Shin EJ, et al. Enteral stenting versus gastrojejunostomy for palliation of malignant gastric outlet obstruction. Surg Endosc. 2013;27:2068–2075. - PubMed
LinkOut - more resources
Full Text Sources
Medical
