

Multiple endo bronchial lipoma: a rare case report
- PMID: 32962678
- PMCID: PMC7510283
- DOI: 10.1186/s12890-020-01287-4
Multiple endo bronchial lipoma: a rare case report
Abstract
Background: Endobronchial lipoma is an extremely rare benign tumor, which is generally located in the first three subdivisions of the tracheobronchial tree. According to the existing literature, all endobronchial lipomas are single (one per patient). Here, we report a rare case in which the patient presented with two endobronchial lipomas in the same patient, and underwent a bronchoscopic tumor resection in the left main bronchus and the left lower bronchus. Both tumors were pathologically confirmed as endobronchial lipoma.
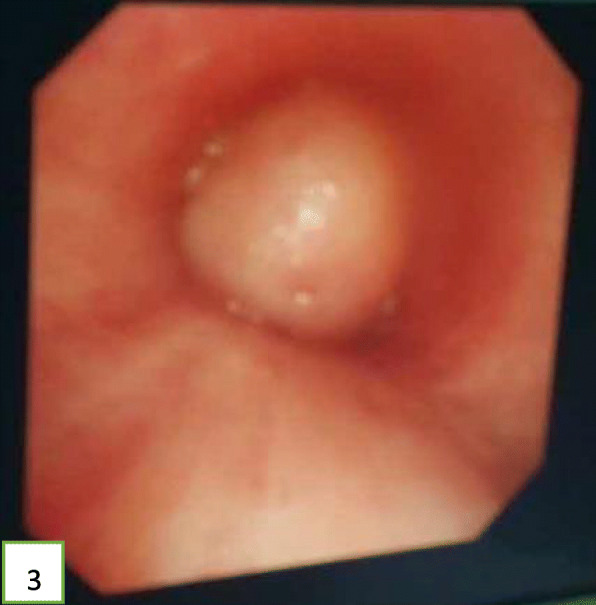
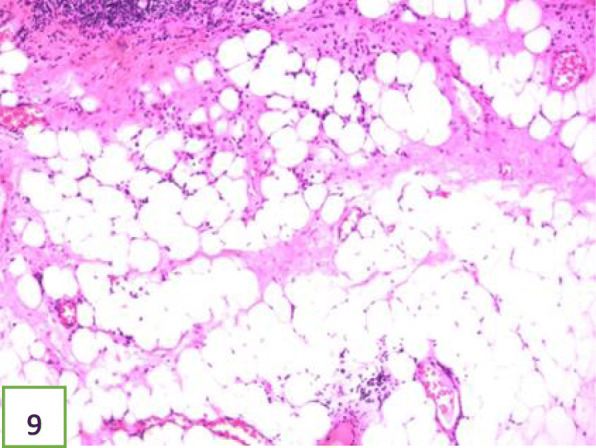
Case presentation: A 52-year-old Chinese man presented at the clinic reporting a mild cough with yellow color sputum and exertional dyspnea for 2 weeks. He was a heavy smoker (45 pack-years). Chest auscultation demonstrated faint wheezing in left lower lobe. Computed tomography (CT) revealed two low-density endobronchial masses located in the middle segment of the left main bronchus and the posterior basilar segmental bronchus of the left lower lobe. The neoplasms measured a CT-attenuation value of -70HU, -98HU in density with air trapping and atelectasis in the segmental bronchus of the left lower lobe. The patient underwent interventional bronchoscopic management to remove the neoplasms by using an electrosurgical snare, cryotherapy, and electrocautery. The locations of the neoplasms were confirmed at the left main bronchus and the superior segment of the left lower lobe during bronchoscopic intervention. Histopathological examination confirmed that both tissues were consistent with lipomas. After 18 months of follow-up, the patient was free of symptoms and CT revealed that bronchiectasia remained in the superior segment of the left lower lobe; however, no mass lesion was present in the left bronchus.
Conclusions: This case suggests that an endobronchial lipoma can present as multiple lesions, and both proximal and distal types can simultaneously occur in the same patient. Thus, these findings help us further understand the biology of endobronchial lipomas.
Keywords: Bronchoscopy; Case report; Endobronchial lipoma; Lipoma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures










References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
