

Dietary mannose supplementation in phosphomannomutase 2 deficiency (PMM2-CDG)
- PMID: 32962735
- PMCID: PMC7510076
- DOI: 10.1186/s13023-020-01528-z
Dietary mannose supplementation in phosphomannomutase 2 deficiency (PMM2-CDG)
Abstract
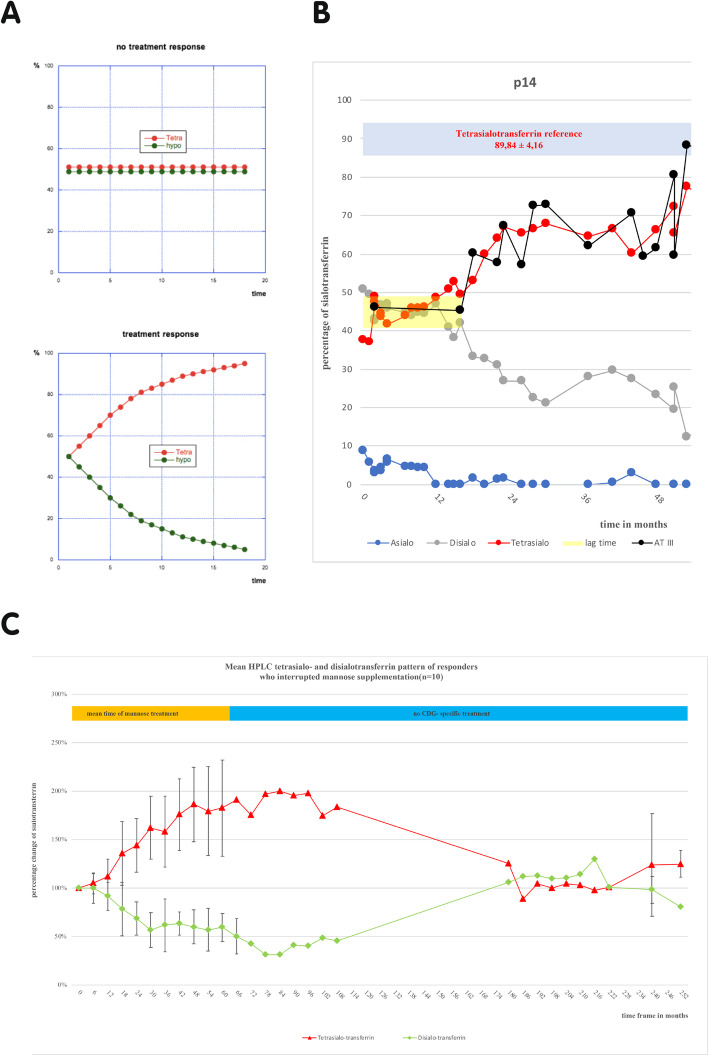
Background: PMM2-CDG (CDG-Ia) is the most frequent N-glycosylation disorder. While supplying mannose to PMM2-deficient fibroblasts corrects the altered N-glycosylation in vitro, short term therapeutic approaches with mannose supplementation in PMM2-CDG patients have been unsuccessful. Mannose found no further mention in the design of a potential therapy for PMM2-CDG in the past years, as it applies to be ineffective. This retrospective study analyzes the first long term mannose supplementation in 20 PMM2-CDG patients. Mannose was given at a total of 1-2 g mannose/kg b.w./d divided into 5 single doses over a mean time of 57,75 ± 25,85 months. Protein glycosylation, blood mannose concentration and clinical presentation were monitored in everyday clinical practice.
Results: After a mean time period of more than 1 year the majority of patients showed significant improvements in protein glycosylation.
Conclusion: Dietary mannose supplementation shows biological effects in PMM2-CDG patients improving glycosylation in the majority of patients. A double-blind randomized study is needed to examine the role of mannose in the design of a therapy for children with PMM2-CDG in more detail.
Keywords: Congenital disorder of glycosylation (CDG); Glycoprotein profile; Mannose; PMM2; Therapy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Comment in
-
Mannose supplementation in PMM2-CDG.Orphanet J Rare Dis. 2021 Aug 11;16(1):359. doi: 10.1186/s13023-021-01988-x. Orphanet J Rare Dis. 2021. PMID: 34380532 Free PMC article.
References
-
- Niehues R, Hasilik M, Alton G, Körner C, Schiebe-Sukumar M, Koch HG, Zimmer KP, Wu R, Harms E, Reiter K, et al. Carbohydrate-deficient glycoprotein syndrome type Ib. Phosphomannose isomerase deficiency and mannose therapy. J Clin Invest. 1998;101:1414–1420. doi: 10.1172/JCI2350. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
