

Risk Factors for Hypervascularization in Hepatobiliary Phase Hypointense Nodules without Arterial Phase Hyperenhancement: A Systematic Review and Meta-analysis
- PMID: 32962925
- PMCID: PMC9115668
- DOI: 10.1016/j.acra.2020.08.031
Risk Factors for Hypervascularization in Hepatobiliary Phase Hypointense Nodules without Arterial Phase Hyperenhancement: A Systematic Review and Meta-analysis
Abstract
Rationale and objectives: To perform a systematic review and meta-analysis to determine risk factors for hypervascularization in hepatobiliary phase (HBP) hypointense nodules without arterial phase hyperenhancement (APHE) in patients with hepatocellular carcinoma (HCC).
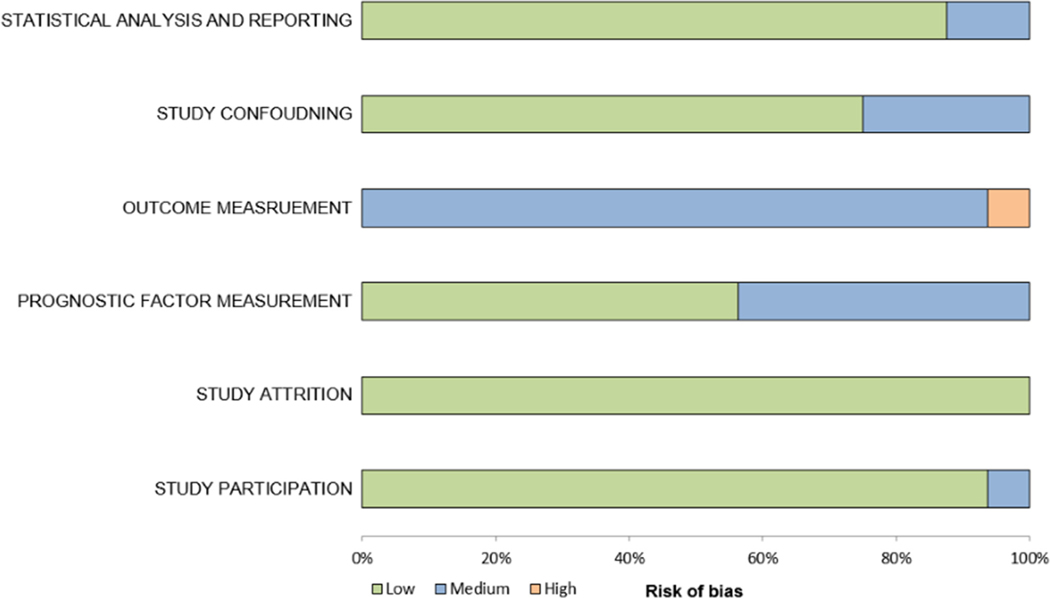
Materials and methods: Pubmed and EMBASE databases were searched up to May 7, 2020. Studies which evaluated radiologic and clinical risk factors for hypervascularization in HBP hypointense nodules without APHE were included. Hazard ratios were meta-analytically pooled using random-effects model. Methodological quality of included studies was assessed using Quality in Prognostic Studies (QUIPS) tool.
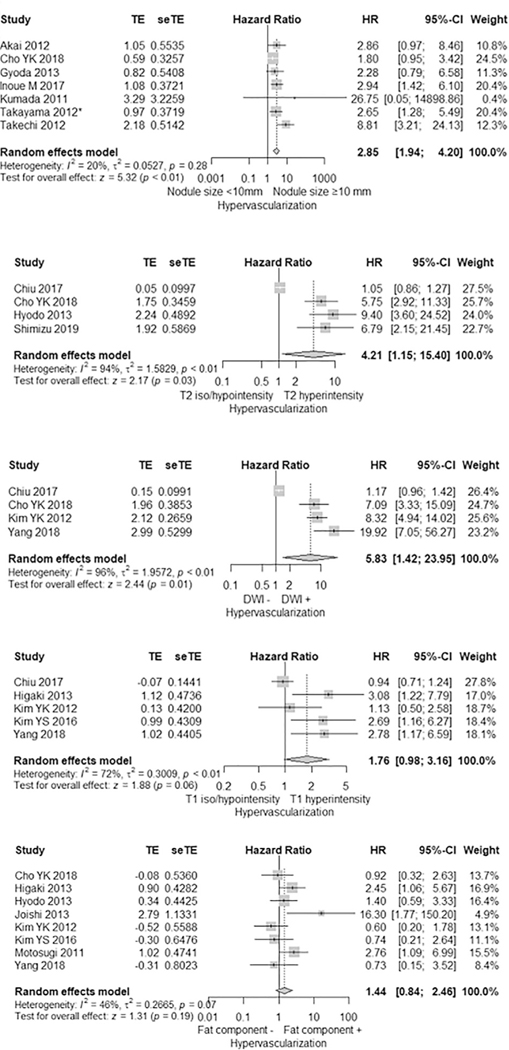
Results: Sixteen studies with 934 patients were included. HBP hypointense nodules without APHE with baseline size greater than 10 mm, T2 hyperintensity, and restricted diffusion showed risk for hypervascularization with pooled HRs of 2.95 (95% confidence interval [CI], 1.94-4.20), 4.21 (95% CI, 1.15-15.40), 5.83 (95% CI, 1.42-23.95), respectively. Previous HCC history contributed to hypervascularization of the nodules with hazard ratio of 2.06 (95% CI, 1.23-3.44). T1 hyperintensity, intralesional fat, Child-Pugh Class B, sex, alfa-fetoprotein, hepatitis B or C infection were not significant risk factors for hypervascularization (p ≥0.05). Study quality was generally moderate.
Conclusion: HBP hypointense nodules without APHE on gadoxetic acid-enhanced MRI with baseline size greater than 10 mm, T2 hyperintensity, restricted diffusion and previous hepatocellular carcinoma history pose higher risk for hypervascularization. Proper patient management in patients with HBP hypointense nodules without APHE on gadoxetic acid-enhanced MRI may need to be tailored according to these risk factors.
Keywords: Arterial phase hyperenhancement; Gd-EOB-DTPA; Hepatocellular carcinoma; Hypervascularization; Meta-analysis; Systematic review.
Copyright © 2020 The Association of University Radiologists. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
DISCLOSURES
There are no conflicts of interest to disclose.
Figures


Comment in
-
Hepatobiliary-Phase Hypointense Nodules without Arterial Phase Hyperenhancement: Time to Act.Acad Radiol. 2022 Feb;29(2):211-212. doi: 10.1016/j.acra.2021.11.018. Epub 2021 Dec 16. Acad Radiol. 2022. PMID: 34922829 No abstract available.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68:394–424. - PubMed
-
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet 2018; 391:1301–1314. - PubMed
-
- EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol 2018; 69:182–236. - PubMed
-
- Marrero JA, Kulik LM, Sirlin CB et al. (2018) Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the study of liver diseases. 68:723–750 - PubMed
-
- Roberts LR, Sirlin CB, Zaiem F, et al. Imaging for the diagnosis of hepatocellular carcinoma: A systematic review and meta-analysis. Hepatology 2018; 67:401–421. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
