

Pulmonary alveolar microlithiasis: no longer in the stone age
- PMID: 32964001
- PMCID: PMC7487355
- DOI: 10.1183/23120541.00289-2020
Pulmonary alveolar microlithiasis: no longer in the stone age
Abstract
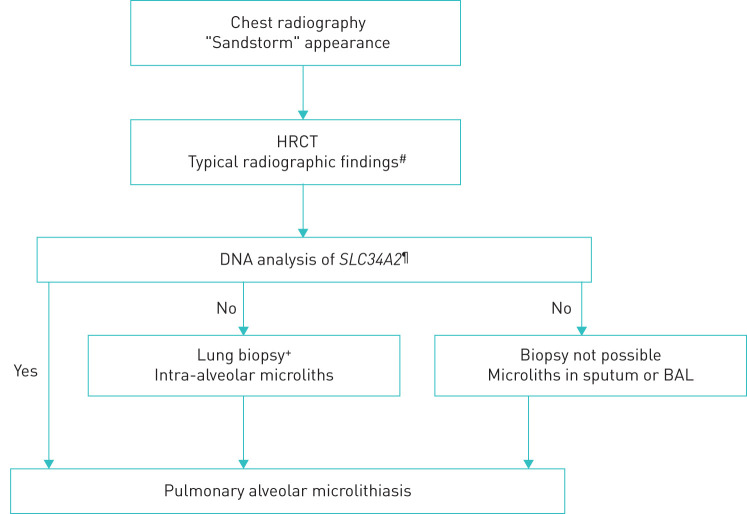
Pulmonary alveolar microlithiasis (PAM) is a rare parenchymal lung disease caused by variants in the SCL34A2 gene and characterised by the accumulation of intra-alveolar microliths. PAM has been reported in fewer than 1100 cases throughout the world. It is an autosomal recessive hereditary disease and often associated with consanguinity. Progress with respect to the genetic background and pathophysiology has resulted in an increased understanding of the disease in recent years. Until now, 30 genetic different SLC34A2 variants have been reported, which all are considered significant for disease development. There is no sex difference and the majority of cases are diagnosed at the age of 30-40 years. Many patients are asymptomatic and the diagnosis is made at random. When symptomatic, dyspnoea, cough, chest pain and fatigue are common complaints. The diagnosis of PAM can confidently be based on typical radiographic findings and genetic testing proving rare biallelic SCL34A2 gene variants. Bronchoalveolar lavage and histopathology may show microliths. There is no disease-specific treatment and management is supportive. Lung transplantation should be considered in advanced cases.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: E. Bendstrup has nothing to disclose. Conflict of interest: Å.L.M. Jönsson has nothing to disclose.
Figures
References
-
- Anzalone M, ed Marcello Malpighi e i suoi scritti sugli organi del respire. Manoscr vol XII, foglio 81 Bologna, Tamari Editori, 1966: pp. 259–262.
-
- Harbitz F. Extensive calcification of the lungs as a distinct disease. Arch Intern Med 1918; 21: 139–146. doi:10.1001/archinte.1918.00090070150012 - DOI
-
- Puhr I. Microlithiasis alveolaris pulmonum. Virchows Arch A Patho Anat Histopathol 1933; 290: 156. doi:10.1007/BF01979722 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous