

Core outcome set for the management of acute exacerbations of chronic obstructive pulmonary disease: the COS-AECOPD ERS Task Force study protocol
- PMID: 32964006
- PMCID: PMC7487360
- DOI: 10.1183/23120541.00193-2020
Core outcome set for the management of acute exacerbations of chronic obstructive pulmonary disease: the COS-AECOPD ERS Task Force study protocol
Abstract
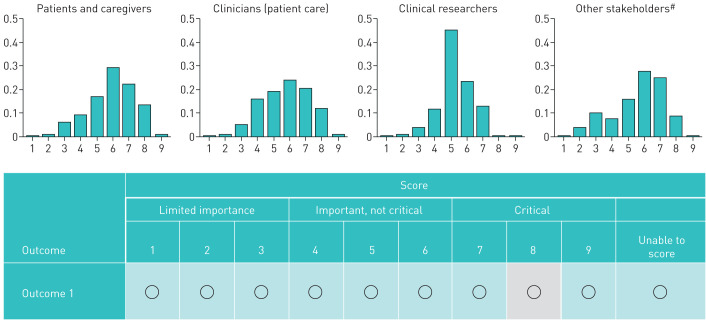
Randomised controlled trials (RCTs) on the management of COPD exacerbations evaluate heterogeneous outcomes, often omitting those that are clinically important and patient relevant. This limits their usability and comparability. A core outcome set (COS) is a consensus-based minimum set of clinically important outcomes that should be evaluated in all RCTs in specific areas of health care. We present the study protocol of the COS-AECOPD ERS Task Force, aiming to develop a COS for COPD exacerbation management, that could remedy these limitations. For the development of this COS we follow standard methodology recommended by the COMET initiative. A comprehensive list of outcomes is assembled through a methodological systematic review of the outcomes reported in relevant RCTs. Qualitative research with patients with COPD will also be conducted, aiming to identify additional outcomes that may be important to patients, but are not currently addressed in clinical research studies. Prioritisation of the core outcomes will be facilitated through an extensive, multi-stakeholder Delphi survey with a global reach. Selection will be finalised in an international, multi-stakeholder meeting. For every core outcome, we will recommend a specific measurement instrument and standardised time points for evaluation. Selection of instruments will be based on evidence-informed consensus. Our work will improve the quality, usability and comparability of future RCTs on the management of COPD exacerbations and, ultimately, the care of patients with COPD. Multi-stakeholder engagement and societal support by the European Respiratory Society will raise awareness and promote implementation of the COS.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: A.G. Mathioudakis reports grants from Boehringer Ingelheim outside the submitted work. Conflict of interest: F. Abroug has nothing to disclose. Conflict of interest: A. Agusti reports personal fees from AstraZeneca, grants and personal fees from Menarini, personal fees from Chiesi, grants and personal fees from GSK, and personal fees from Nuvaira, outside the submitted work. Conflict of interest: P. Bakke reports personal fees from GlaxoSmithKline, Chiesi, AstraZeneca and Boehringer Ingelheim outside the submitted work. Conflict of interest: K. Bartziokas has nothing to disclose. Conflict of interest: B. Beghe has nothing to disclose. Conflict of interest: A. Bikov has nothing to disclose. Conflict of interest: T. Bradbury reports being the recipient of an ongoing 3-year top-up scholarship funded by GlaxoSmithKline. Conflict of interest: G. Brusselle reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Sanofi and Teva, outside the submitted work. Conflict of interest: C. Cadus reports support from AstraZeneca and Mundipharma, outside the submitted work. Conflict of interest: C. Coleman is an employee of the European Lung Foundation. Conflict of interest: M. Contoli reports grants from Chiesi, personal fees from Chiesi, AstraZeneca, Boehringer Ingelheim, ALK-Abello, Novartis and Zambon, and grants from University of Ferrara, outside the submitted work. Conflict of interest: A. Corlateanu has nothing to disclose. Conflict of interest: O. Corlateanu has nothing to disclose. Conflict of interest: G. Criner has nothing to disclose. Conflict of interest: B. Csoma has nothing to disclose. Conflict of interest: A. Emelyanov has nothing to disclose. Conflict of interest: R. Faner reports grants from GSK and Menarini outside the submitted work. Conflict of interest: G. Fernandez Romero has nothing to disclose. Conflict of interest: Z. Hammouda has nothing to disclose. Conflict of interest: P. Horváth has nothing to disclose. Conflict of interest: A. Huerta Garcia has nothing to disclose. Conflict of interest: M. Jacobs has nothing to disclose. Conflict of interest: C. Jenkins has nothing to disclose. Conflict of interest: G. Joos reports grants and personal fees from AstraZeneca, personal fees from Bayer, grants from Chiesi, personal fees from Eureca vzw, grants and personal fees from GlaxoSmithKline and personal fees from Teva, outside the submitted work; these grants and fees were paid to his institution. Conflict of interest: O. Kharevich has nothing to disclose. Conflict of interest: K. Kostikas reports grants, personal fees and nonfinancial support from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, Menarini and Novartis, grants from NuvoAir, and personal fees from Sanofi, outside the submitted work; and was an employee and shareholder of Novartis Pharma AG until 31 October 2018. Conflict of interest: E. Lapteva has nothing to disclose. Conflict of interest: Z. Lazar has nothing to disclose. Conflict of interest: J.D. Leuppi has nothing to disclose. Conflict of interest: C. Liddle has nothing to disclose. Conflict of interest: A. López-Giraldo has nothing to disclose. Conflict of interest: V.M. McDonald reports grants and personal fees from GSK and AstraZeneca, and personal fees from Menarini, outside the submitted work. Conflict of interest: R. Nielsen reports grants and personal fees from AstraZeneca and Boehringer Ingelheim, grants from Novartis, and grants and personal fees from GlaxoSmithKline, outside the submitted work. Conflict of interest: A. Papi reports grants, personal fees, nonfinancial support and other from GlaxoSmithKline; grants, personal fees and nonfinancial support from AstraZeneca; grants, personal fees, nonfinancial support and other from Boehringer Ingelheim; grants, personal fees, nonfinancial support and other from Chiesi Farmaceutici; grants, personal fees, nonfinancial support and other from TEVA; personal fees, non-financial support and other from Mundipharma; personal fees, non-financial support and other from Zambon; personal fees, non-financial support and other from Novartis; grants, personal fees and non-financial support from Menarini; personal fees, non-financial support and other from Sanofi/Regeneron; personal fees from Roche; grants from Fondazione Maugeri; grants from Fondazione Chiesi; and personal fees from Edmondpharma, all outside the submitted work. Conflict of interest: I. Saraiva has nothing to disclose. Conflict of interest: G. Sergeeva has nothing to disclose. Conflict of interest: A. Sioutkou has nothing to disclose. Conflict of interest: P. Sivapalan reports personal fees from Boehringer Ingelheim outside the submitted work. Conflict of interest: E. Stovold has nothing to disclose. Conflict of interest: H. Wang has nothing to disclose. Conflict of interest: F. Wen has nothing to disclose. Conflict of interest: J. Yorke has nothing to disclose. Conflict of interest: P.R. Williamson has nothing to disclose. Conflict of interest: J. Vestbo reports personal fees from AstraZeneca, grants and personal fees from Boehringer-Ingelheim, personal fees from Chiesi, personal fees from GSK, and personal fees from Novartis, outside the submitted work; and his son is an employee of Chiesi. Conflict of interest: J-U. Jensen has nothing to disclose.
Figures
Similar articles
-
ERS statement: a core outcome set for clinical trials evaluating the management of COPD exacerbations.Eur Respir J. 2022 May 5;59(5):2102006. doi: 10.1183/13993003.02006-2021. Print 2022 May. Eur Respir J. 2022. PMID: 34649975
-
IMMPACT-recommended outcome measures and tools of assessment in burning mouth syndrome RCTs: an international Delphi survey protocol.Trials. 2020 Aug 12;21(1):711. doi: 10.1186/s13063-020-04640-4. Trials. 2020. PMID: 32787910 Free PMC article.
-
Protocol for the development of a core outcome set for pelvic girdle pain, including methods for measuring the outcomes: the PGP-COS study.BMC Med Res Methodol. 2018 Dec 3;18(1):158. doi: 10.1186/s12874-018-0624-5. BMC Med Res Methodol. 2018. PMID: 30509216 Free PMC article.
-
Harmonisation of Outcome Parameters and Evaluation (HOPE) for actinic keratosis: protocol for the development of a core outcome set.Trials. 2019 Oct 11;20(1):589. doi: 10.1186/s13063-019-3696-6. Trials. 2019. PMID: 31604473 Free PMC article.
-
Development of a core outcome set for clinical trials in facial aging: study protocol for a systematic review of the literature and identification of a core outcome set using a Delphi survey.Trials. 2017 Aug 1;18(1):359. doi: 10.1186/s13063-017-2104-3. Trials. 2017. PMID: 28764734 Free PMC article.
Cited by
-
Predictors of treatment REsponse to inhaled corticosteroids (ICS) in Chronic Obstructive pulmonary disease: randomised controlled trials individual participant Data re-Evaluation-protocol of the ICS-RECODE individual participant data meta-analysis.BMJ Open. 2025 Mar 5;15(3):e095541. doi: 10.1136/bmjopen-2024-095541. BMJ Open. 2025. PMID: 40044194 Free PMC article.
-
Inspiring stories: the impact that being part of ERS activities can have on a professional career.Breathe (Sheff). 2022 Mar;18(1):210217. doi: 10.1183/20734735.0217-2021. Epub 2021 Mar 8. Breathe (Sheff). 2022. PMID: 35284021 Free PMC article.
-
Assessing Treatment Success or Failure as an Outcome in Randomised Clinical Trials of COPD Exacerbations. A Meta-Epidemiological Study.Biomedicines. 2021 Dec 5;9(12):1837. doi: 10.3390/biomedicines9121837. Biomedicines. 2021. PMID: 34944653 Free PMC article.
-
Outcomes Evaluated in Controlled Clinical Trials on the Management of COVID-19: A Methodological Systematic Review.Life (Basel). 2020 Dec 15;10(12):350. doi: 10.3390/life10120350. Life (Basel). 2020. PMID: 33333777 Free PMC article.
-
Current developments and future directions in COPD.Eur Respir Rev. 2020 Dec 2;29(158):200289. doi: 10.1183/16000617.0289-2020. Print 2020 Dec 31. Eur Respir Rev. 2020. PMID: 33268439 Free PMC article.
References
-
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med 2017; 5: 691–706. doi:10.1016/S2213-2600(17)30293-X - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources