

Decision-making in the diagnosis of tuberculous meningitis
- PMID: 32964134
- PMCID: PMC7490569
- DOI: 10.12688/wellcomeopenres.15611.1
Decision-making in the diagnosis of tuberculous meningitis
Abstract
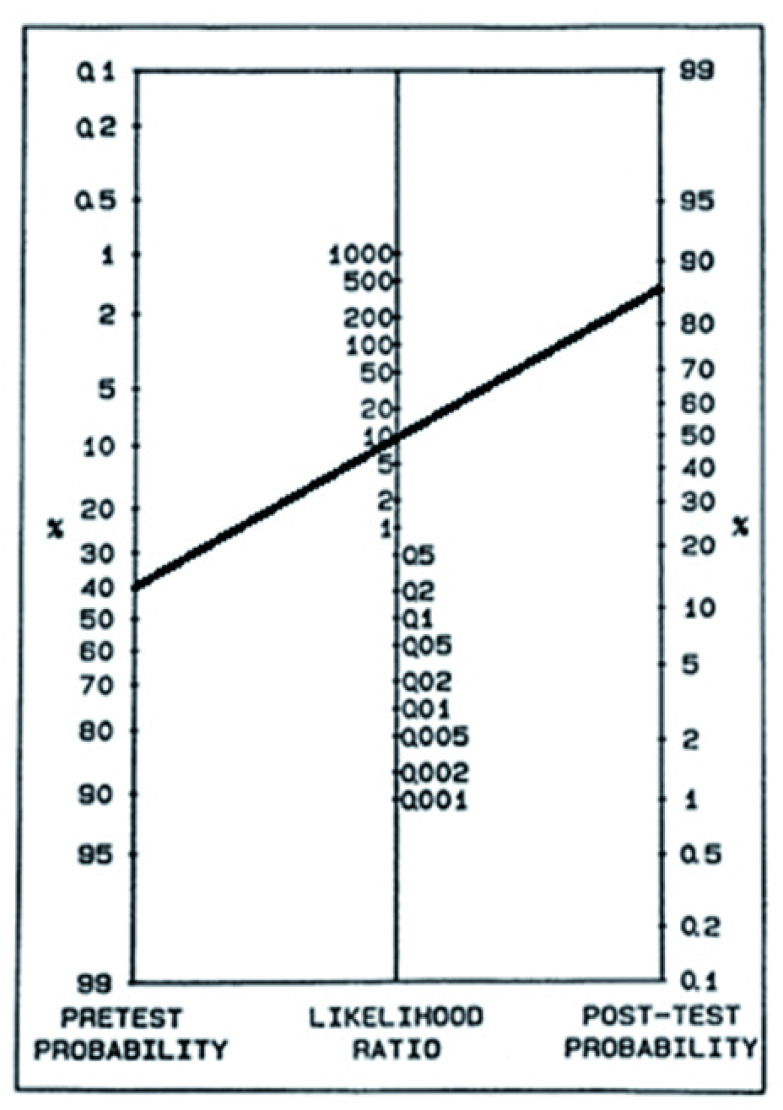
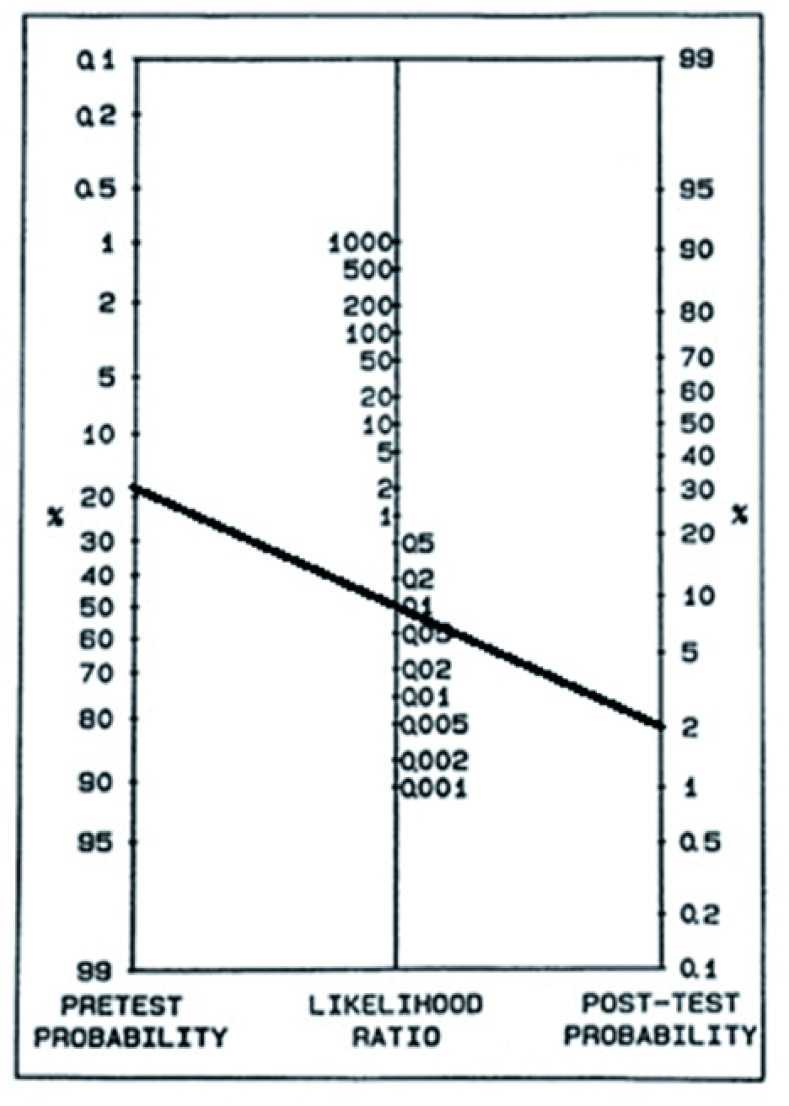
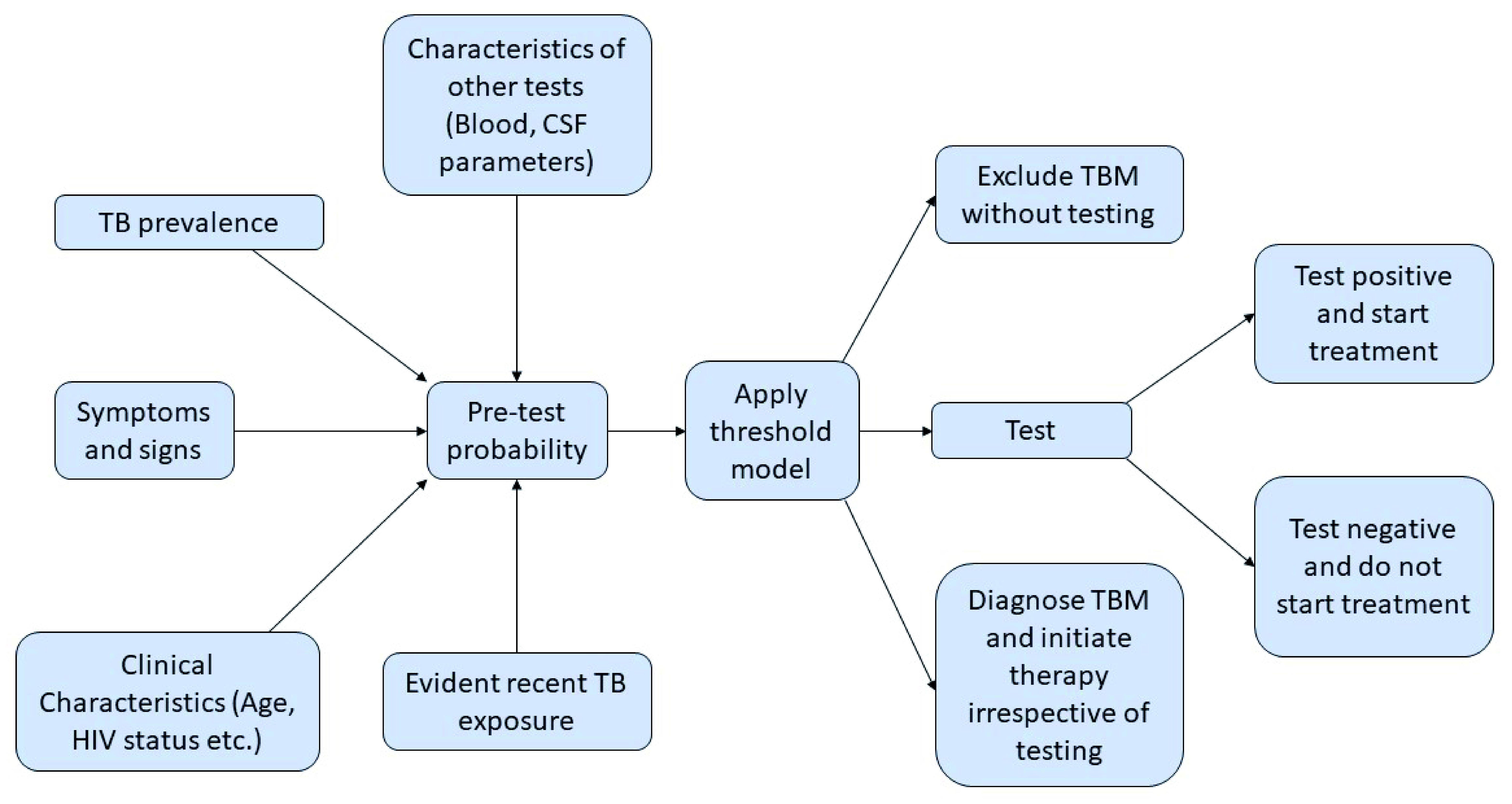
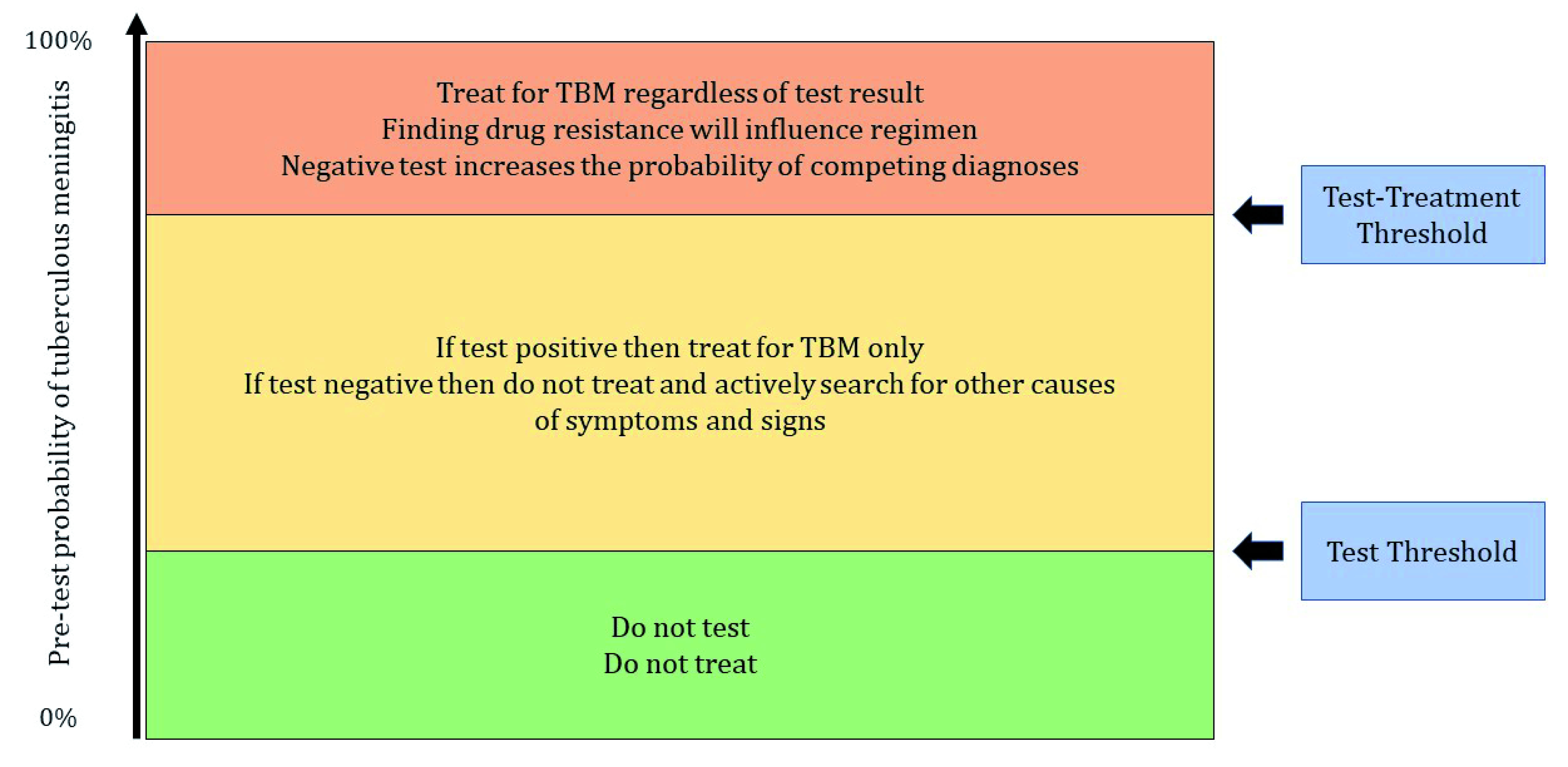
Tuberculous meningitis (TBM) is the most devastating form of tuberculosis (TB) but diagnosis is difficult and delays in initiating therapy increase mortality. All currently available tests are imperfect; culture of Mycobacterium tuberculosis from the cerebrospinal fluid (CSF) is considered the most accurate test but is often negative, even when disease is present, and takes too long to be useful for immediate decision making. Rapid tests that are frequently used are conventional Ziehl-Neelsen staining and nucleic acid amplification tests such as Xpert MTB/RIF and Xpert MTB/RIF Ultra. While positive results will often confirm the diagnosis, negative tests frequently provide insufficient evidence to withhold therapy. The conventional diagnostic approach is to determine the probability of TBM using experience and intuition, based on prevalence of TB, history, examination, analysis of basic blood and CSF parameters, imaging, and rapid test results. Treatment decisions may therefore be both variable and inaccurate, depend on the experience of the clinician, and requests for tests may be inappropriate. In this article we discuss the use of Bayes' theorem and the threshold model of decision making as ways to improve testing and treatment decisions in TBM. Bayes' theorem describes the process of converting the pre-test probability of disease to the post-test probability based on test results and the threshold model guides clinicians to make rational test and treatment decisions. We discuss the advantages and limitations of using these methods and suggest that new diagnostic strategies should ultimately be tested in randomised trials.
Keywords: Tuberculosis Meningitis Diagnosis Threshold Decision.
Copyright: © 2020 Boyles TH et al.
Conflict of interest statement
No competing interests were disclosed.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
