

Assessing a novel, lab-free, point-of-care test for SARS-CoV-2 (CovidNudge): a diagnostic accuracy study
- PMID: 32964211
- PMCID: PMC7498257
- DOI: 10.1016/S2666-5247(20)30121-X
Assessing a novel, lab-free, point-of-care test for SARS-CoV-2 (CovidNudge): a diagnostic accuracy study
Erratum in
-
Correction to Lancet Microbe 2020; 1: e300-07.Lancet Microbe. 2020 Nov;1(7):e280. doi: 10.1016/S2666-5247(20)30174-9. Epub 2020 Nov 4. Lancet Microbe. 2020. PMID: 33521727 Free PMC article.
Abstract
Background: Access to rapid diagnosis is key to the control and management of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Laboratory RT-PCR testing is the current standard of care but usually requires a centralised laboratory and significant infrastructure. We describe our diagnostic accuracy assessment of a novel, rapid point-of-care real time RT-PCR CovidNudge test, which requires no laboratory handling or sample pre-processing.
Methods: Between April and May, 2020, we obtained two nasopharyngeal swab samples from individuals in three hospitals in London and Oxford (UK). Samples were collected from three groups: self-referred health-care workers with suspected COVID-19; patients attending emergency departments with suspected COVID-19; and hospital inpatient admissions with or without suspected COVID-19. For the CovidNudge test, nasopharyngeal swabs were inserted directly into a cartridge which contains all reagents and components required for RT-PCR reactions, including multiple technical replicates of seven SARS-CoV-2 gene targets (rdrp1, rdrp2, e-gene, n-gene, n1, n2 and n3) and human ribonuclease P (RNaseP) as sample adequacy control. Swab samples were tested in parallel using the CovidNudge platform, and with standard laboratory RT-PCR using swabs in viral transport medium for processing in a central laboratory. The primary analysis was to compare the sensitivity and specificity of the point-of-care CovidNudge test with laboratory-based testing.
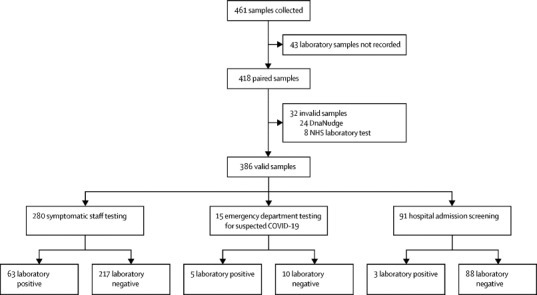
Findings: We obtained 386 paired samples: 280 (73%) from self-referred health-care workers, 15 (4%) from patients in the emergency department, and 91 (23%) hospital inpatient admissions. Of the 386 paired samples, 67 tested positive on the CovidNudge point-of-care platform and 71 with standard laboratory RT-PCR. The overall sensitivity of the point-of-care test compared with laboratory-based testing was 94% (95% CI 86-98) with an overall specificity of 100% (99-100). The sensitivity of the test varied by group (self-referred healthcare workers 94% [95% CI 85-98]; patients in the emergency department 100% [48-100]; and hospital inpatient admissions 100% [29-100]). Specificity was consistent between groups (self-referred health-care workers 100% [95% CI 98-100]; patients in the emergency department 100% [69-100]; and hospital inpatient admissions 100% [96-100]). Point of care testing performance was similar during a period of high background prevalence of laboratory positive tests (25% [95% 20-31] in April, 2020) and low prevalence (3% [95% 1-9] in inpatient screening). Amplification of viral nucleocapsid (n1, n2, and n3) and envelope protein gene (e-gene) were most sensitive for detection of spiked SARS-CoV-2 RNA.
Interpretation: The CovidNudge platform was a sensitive, specific, and rapid point of care test for the presence of SARS-CoV-2 without laboratory handling or sample pre-processing. The device, which has been implemented in UK hospitals since May, 2020, could enable rapid decisions for clinical care and testing programmes.
Funding: National Institute of Health Research (NIHR) Imperial Biomedical Research Centre, NIHR Health Protection Research Unit in Healthcare Associated Infections and Antimicrobial Resistance at Oxford University in partnership with Public Health England, NIHR Biomedical Research Centre Oxford, and DnaNudge.
© 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license.
Figures

Comment in
-
Innovative point-of-care molecular diagnostic test for COVID-19 in India.Lancet Microbe. 2020 Nov;1(7):e277. doi: 10.1016/S2666-5247(20)30164-6. Epub 2020 Nov 4. Lancet Microbe. 2020. PMID: 33521725 Free PMC article. No abstract available.
References
-
- Johns Hopinks University COVID-19 Map—Johns Hopkins Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html
-
- He X, Lau EH, Wu P. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020;26:672–675. - PubMed
-
- Wölfel R, Corman VM, Guggemos W. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020;581:465–469. - PubMed
Uncited References
-
- NHS England Guidance and standard operating procedure COVID-19 virus testing in NHS laboratories. https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
