

Frequent premature ventricular contractions. Association of burden and complexity with prognosis according to the presence of structural heart disease
- PMID: 32964593
- PMCID: PMC7816816
- DOI: 10.1111/anec.12800
Frequent premature ventricular contractions. Association of burden and complexity with prognosis according to the presence of structural heart disease
Abstract
Introduction: Premature ventricular contractions (PVC) have been associated with mortality and heart failure (HF) regardless the presence of structural heart disease (SHD). The aim of this study was assessing the impact of burden and complexity of PVCs on prognosis, according to presence of SHD.
Methods: 312 patients were retrospectively evaluated out of 1967 consecutive patients referred for 24-hr Holter at a single hospital, with a PVC count >1% of total beats. Two groups with and without SHD. PVC burden (PVC%), presence of complex forms, incidence of all-cause death, combined outcomes of all-cause death and cardiovascular hospitalizations, HF death and HF hospitalizations and, sudden death (SD) or hospitalizations due to ventricular arrhythmias (VA)were assessed.
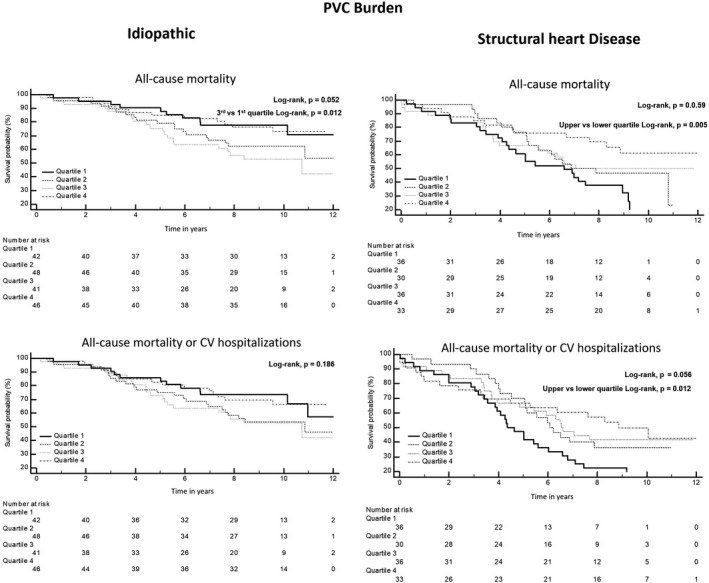
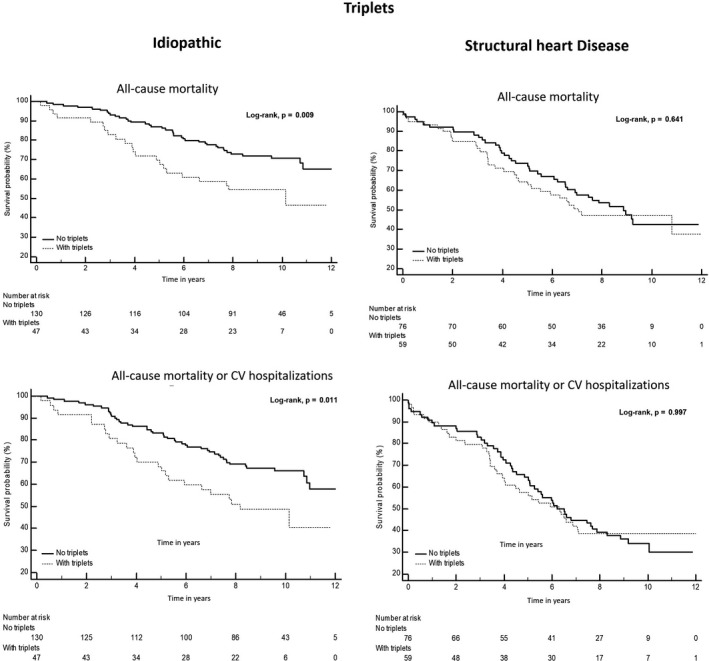
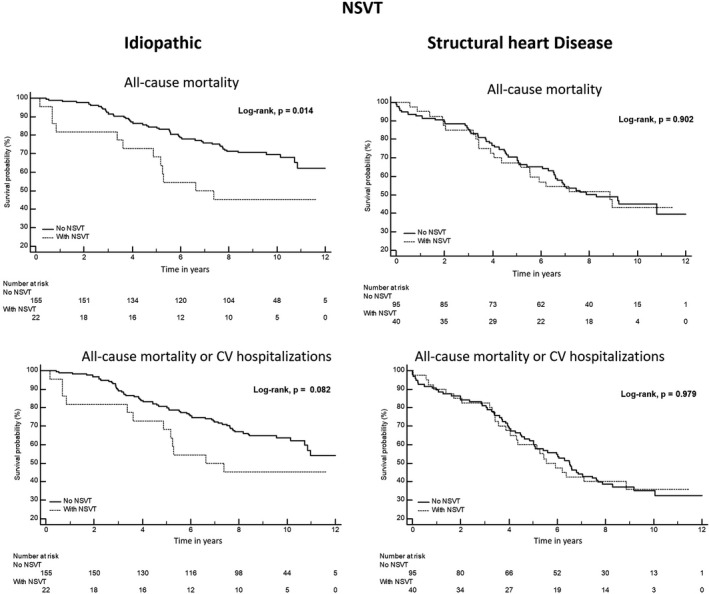
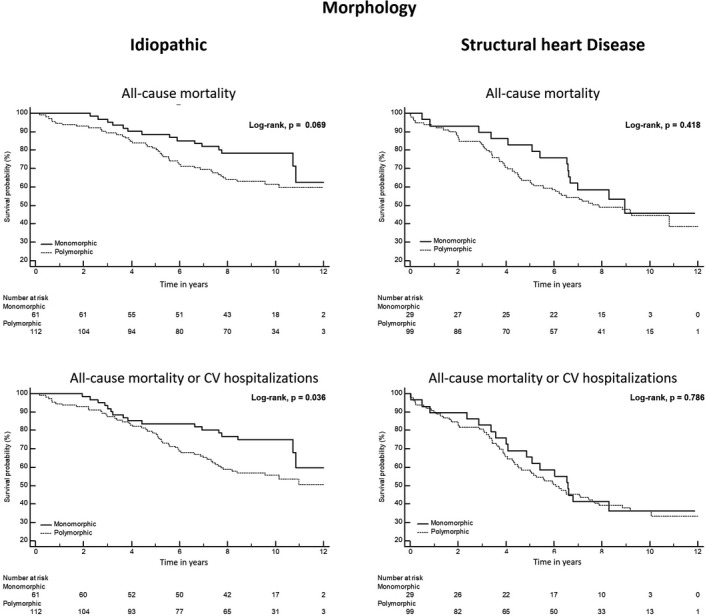
Results: Premature ventricular contraction burden was 2.7 (IQR: 1.6-6.7). SHD patients had more polymorphic PVCs, 77% versus 65%, p = .022, triplets and episodes of non-sustained ventricular tachycardia (NSVT): 44% versus 27%, p = .002; 30% versus 12%, p < .0001. In idiopathic patients, a PVC% in the third quartile was independently associated with all-cause mortality hazard ratio (HR) 2.288 (1.042-5.026) p = .039, but not in SHD. The complexity of the PVCs was not independently associated with outcomes in both groups. In SHD group, NSVT was associated with lower survival free from SD and VA hospitalizations, p = .028; after multivariable, there was a trend for a higher arrhythmic outcome with NSVT, HR 3.896 (0.903-16.81) p = .068.
Conclusion: Premature ventricular contractions in SHD showed more complex patterns. In idiopathic patients, a higher PVC count was associated with higher mortality but not is SHD patients. Complexity was not independently associated with worse prognosis.
Keywords: PVC burden; PVC complexity; idiopathic; premature ventricular contractions; prognosis; structural heart disease.
© 2020 The Authors. Annals of Noninvasive Electrocardiology published by Wiley Periodicals LLC.
Conflict of interest statement
None declared.
Figures
References
-
- Agarwal, S. , Simpson, R. , Rautaharju, P. , Alonso, A. , Shahar, E. , Massing, M. , … Heiss, G. (2012). Relationship of ventricular premature complexes to heart failure (from the Atherosclerosis Risk in Communities [ARIC] study). American Journal of Cardiology, 109, 105–109. 10.1016/j.amjcard.2011.08.009 - DOI - PMC - PubMed
-
- Al‐Khatib, S. , Stevenson, W. , Ackerman, M. , Bryant, W. , Callan, D. , Curtis, A. , … Page, R..(2018). 2017 AHA/ACC/HRS guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation, 138, e272–e391. 10.1161/CIR.0000000000000549 - DOI - PubMed
-
- Arnar, D. O. , Mairesse, G. H. , Boriani, G. , Calkins, H. , Chin, A. , Coats, A. , … Heinzel, F. R. (2019). Management of asymptomatic arrhythmias: A European Heart Rhythm Association (EHRA)consensus document, endorsed by the Heart Failure Association (HFA), Heart Rhythm Society (HRS), Asia Pacific Heart Rhythm Society (APHRS), Cardiac Arrhythmia Society of Southern Africa (CASSA), and Latin America Heart Rhythm Society (LAHRS). Europace, 1–32. 10.1093/europace/euz046 - DOI - PubMed
-
- Baman, T. S. , Lange, D. C. , Ilg, K. J. , Gupta, S. K. , Liu, T.‐Y. , Alguire, C. , … Bogun, F. (2010). Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm: the Official Journal of the Heart Rhythm Society, 7, 865–869. 10.1016/j.hrthm.2010.03.036 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
